RPA is already the backbone of healthcare automation and for good reason. Most healthcare organizations rely on it to run predictable, high-volume clinical and administrative tasks at scale. But a new shift is underway.
As agentic AI accelerates, automation is no longer just about executing rules. It’s about reasoning, adapting, and making decisions across complex clinical workflows. That changes everything.
Healthcare and digital leaders who already use RPA and now face a bigger question: how to evolve automation without breaking what already works. We’ll unpack the real distinction between RPA and agentic AI – not as a technical debate, but as an architectural choice that will shape the next generation of clinical operations.
The question is no longer what can be automated.
It’s where RPA should remain and where agentic AI must take the lead.
RPA automates clicks; Agentic AI automates decisions. Where RPA breaks the moment a payer rule changes or a workflow shifts, Agentic AI reads clinical context, adapts, and executes multi-step tasks end-to-end, no human fixing exceptions, no new bot for every edge case. The workflows driving the most burnout and revenue leakage are exactly the ones RPA was never built to handle.
Handling High-Volume Repetitive Workflows with RPA
What RPA Consists of and How it Functions
Robotic Process Automation is a software technology that mimics human interactions with digital systems. It follows deterministic, pre-defined rule sets to move data, trigger actions, and execute workflows across applications without modifying the underlying systems it operates within.
The global RPA in healthcare market is estimated at $2.80 billion in 2025 and projected to reach $22.56 billion by 2034 at a CAGR of 26.1%. The healthcare and pharma segment is among the fastest-growing verticals in the broader RPA market.
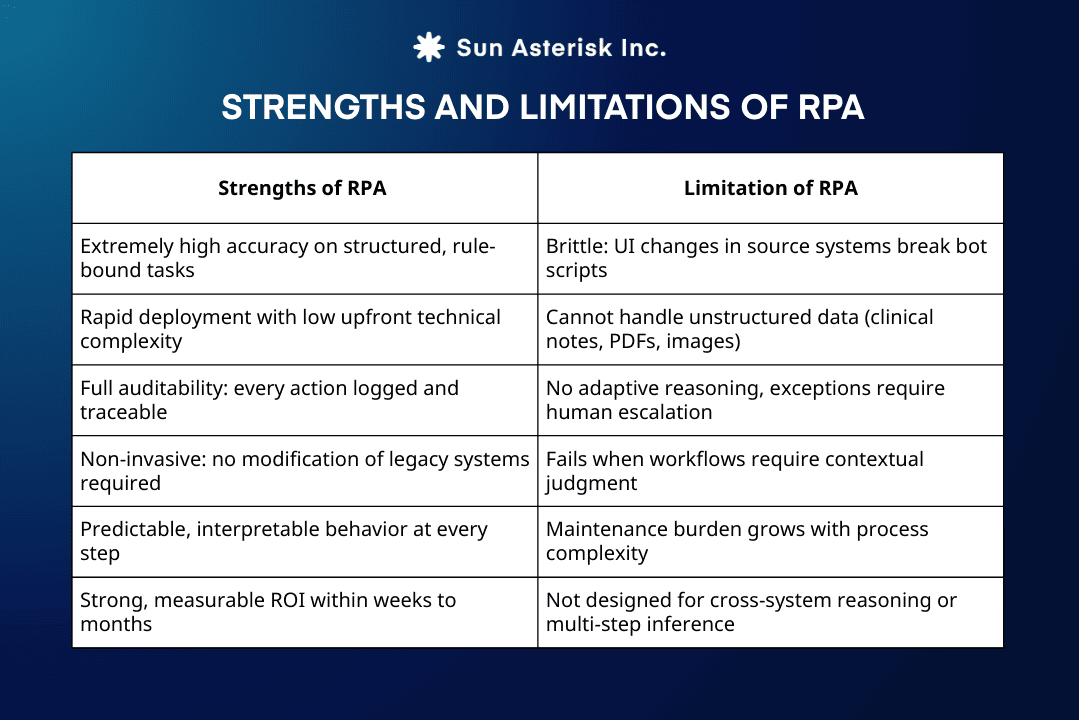
Unlike AI, RPA does not learn from unstructured data or adapt to novel situations. It executes with exactitude what it was instructed to do, every time.
Who Needs RPA and When to Deploy It?
RPA is the right tool when the task is well-defined, the data is structured, and variation is minimal. The clearest signal: if a clinician or administrator can describe the exact steps they take.
In sequence, without ambiguity, RPA can execute that process at scale, with perfect consistency.
RPA delivers the most value in clinical environments where volume, structure, and predictability dominate the workflow. It is purpose-built for operations that require consistent execution across systems, claims submission and tracking, eligibility checks at intake, demographic data entry across EHRs, appointment confirmations, lab result routing, and regulatory reporting.

The primary beneficiaries are teams measured on throughput and accuracy: revenue cycle and coding departments processing thousands of claims and ICD codes, health plan operations verifying member eligibility, ambulatory practices managing referral intake, labs and radiology units distributing structured reports, and IT or compliance teams aggregating audit data.
The signal to deploy RPA is clear: when the work is rule-driven, repeatable, and tolerant of little ambiguity, RPA excels. It is not about replacing judgment. It is about industrializing reliability where logic is fixed and scale is the constraint.
Navigating Complex Clinical Workflows with Agentic AI
Understanding the Agentic Workflow Infrastructure
An AI agent is an autonomous software system capable of perceiving its environment, reasoning across multi-step problems, taking actions, and learning from outcomes without requiring explicit instructions for each step.
In healthcare, this means an agent can read a discharge summary, cross-reference treatment guidelines, identify a gap in care coordination, and trigger the appropriate follow-up workflow. All without a human mapping each decision point.
Agentic AI systems in clinical contexts are built on several interconnected layers.
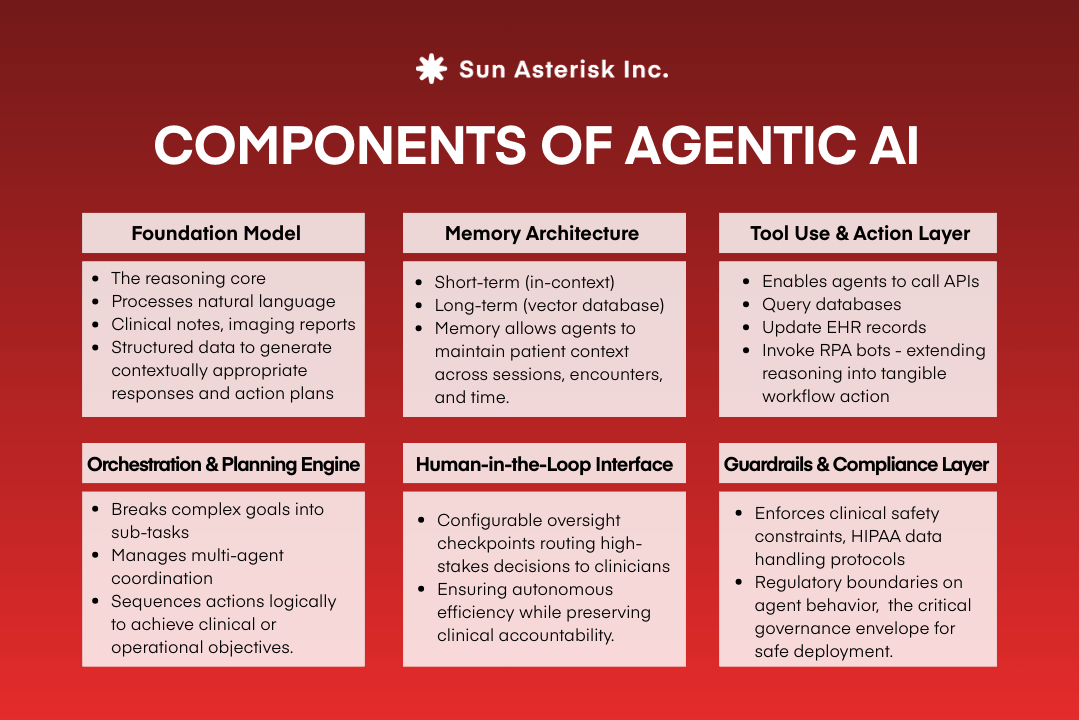
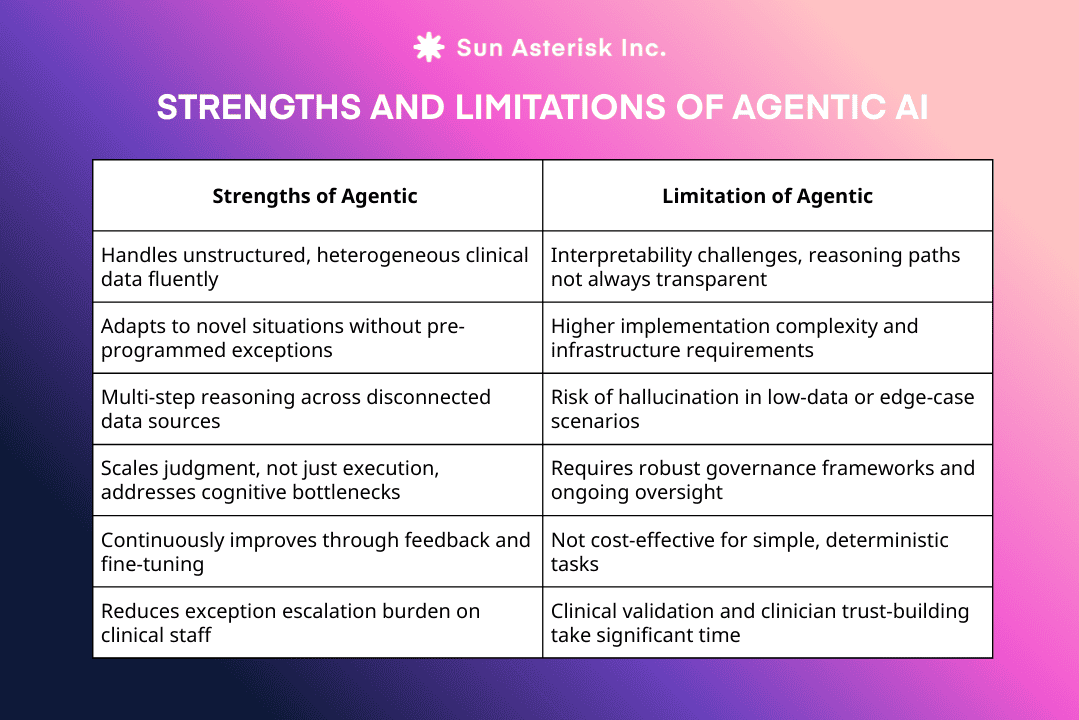
Agent AI can capture unsorted data and handle any data structure; however, it still faces many issues related to compliance, cost, and interpretability.
Why Clinicians Need Agentic Autonomy?
The workflows where healthcare organizations experience the most friction are rarely the ones that reduce to a flowchart.
They involve judgment: prioritizing a complex patient for specialist referral, synthesizing contradictory clinical documentation, adapting a care pathway when a patient’s condition evolves mid-cycle. These are not tasks RPA can address and they are precisely where Agentic AI creates transformative value.
- Reduce healthcare burden: The administrative toll in healthcare is stark. The 2024 survey by the American Medical Association shows physicians manage 39 prior authorizations per week, spending 13 hours on paperwork. 89% link it to burnout, 93% to delayed care, and 40% of practices now hire staff solely for this task. This is the operational strain agentic AI is built to remove by automating decisions, not just documentation.
- ROI: A 2025 peer-reviewed study in Frontiers in Medicine estimated a $1.78M five-year investment in a hospital AI platform, delivering a 451% ROI, with 335% ROI realized within the first year. ROI is no longer a future promise, it’s becoming an operating assumption.
- Improve customer experience & system productivity: Confidence in agentic AI is outpacing deployment. January 2026 research in the New England Journal of Medicine shows only 3% of health systems use agentic AI live, yet 60% expect better provider–patient experiences and 57% expect productivity gains.
Read more: AI Agents in healthcare: How Agentic Documentation Powers Clinical Reasoning
Key differences between RPA and Agentic Workflows in clinical industry
The RPA vs. Agentic AI debate is sometimes framed as old and new. That framing misses the point. These are complementary tools with distinct operating envelopes. The comparison below is grounded in both technical architecture and clinical operational reality:
| Dimension | RPA | Agentic AI |
|---|---|---|
| Core function | Task execution via rule-based automation | Goal-directed reasoning and adaptive action |
| Data type handled | Structured, formatted data only | Structured, unstructured, and multimodal data |
| Decision logic | Deterministic (if/then rules) | Probabilistic (contextual inference) |
| Exception handling | Escalates to humans; limited self-recovery | Reasons through exceptions autonomously |
| Setup complexity | Low – visual scripting, rapid deployment | High-model selection, fine-tuning, governance |
| Interpretability | Fully transparent, complete audit trail | Partially interpretable requires explainability frameworks |
| Adaptability | Static requires manual update for process changes | Dynamic adapts to new information and context |
| Best clinical use cases | Claims, eligibility, scheduling, data entry | Prior authority reasoning, clinical summarization, care gaps, denials |
| Regulatory compliance | Well-established patterns (HIPAA, SOC 2) | Emerging governance; active management required |
| ROI timeline | Short weeks to months | Medium to long months; significantly higher ceiling |
Will Agents AI replace RPA in healthcare?
This question surfaces in every health system strategy meeting where automation is on the agenda.
The answer – grounded in both the technical realities and the operational evidence – is no. But the nuance matters enormously.
The “replacement” narrative assumes that Agentic AI can do everything RPA does, only better. This is architecturally incorrect. Agentic AI is not a superior form of RPA, it’s a different category of tool, operating at a different cognitive layer. Deploying an AI agent to submit a routine claim status inquiry introduces latency, cost, and interpretability risk into a task that a deterministic bot handles with perfect reliability in seconds.
What is actually happening and what forward-thinking healthcare organizations are already designing for, is a repositioning.
RPA is moving from being the primary automation layer to being a precision execution engine within a broader, agent-orchestrated ecosystem. Agents reason and plan; bots execute with exactitude. Neither can fully substitute for the other.
Hybrid Automation: How RPA and Agentic Workflows work together?
Why does this hybrid model work?
The hybrid model works because it respects the cognitive architecture of clinical work.
Clinical workflows are not uniformly complex; they contain zones of pure structure (data entry, format conversion, status polling) and zones of genuine ambiguity (clinical synthesis, exception reasoning, multi-criteria prioritization).
A single automation layer cannot serve both zones optimally.
How does it work in practice?
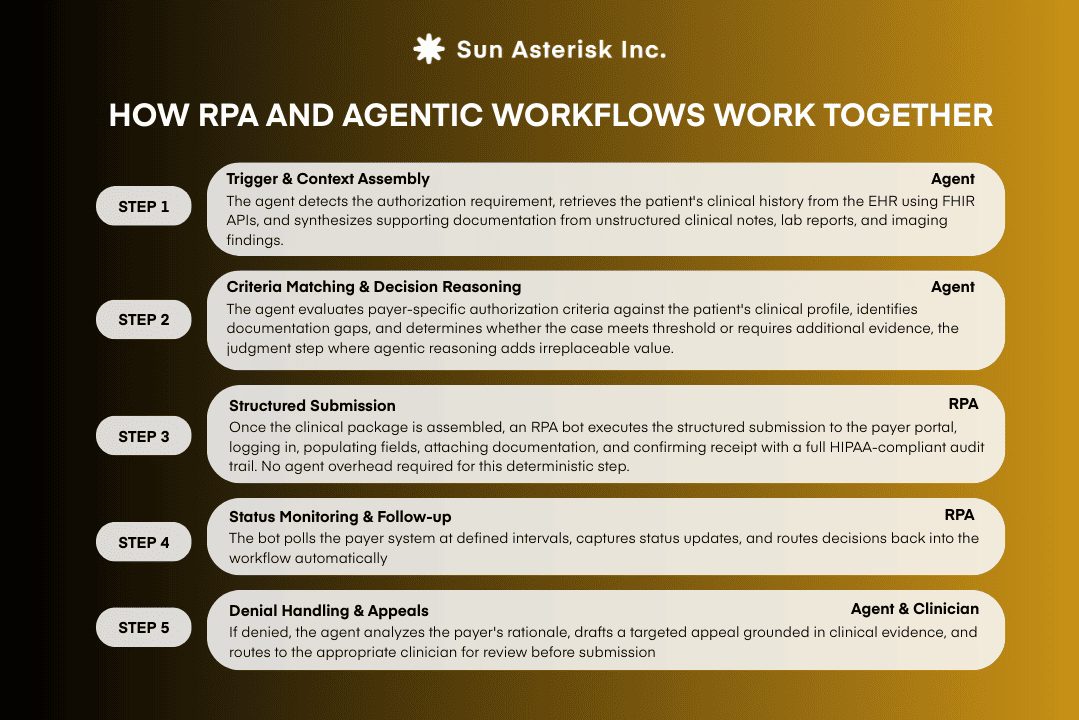
Consider a prior authorization workflow, one of the most friction-intensive processes in U.S. healthcare.
Per the AMA’s 2024 survey, physicians spend 13 hours weekly on prior authorization, 93% report it delays care, and 1 in 3 physicians say their requests are often or always denied.
This is exactly the workflow a hybrid architecture is designed to transform:
How to balance between RPA and agentic workflows?
Balancing RPA and agentic AI isn’t a choice between two technologies, it’s about using each where it delivers the most value.
RPA is best suited for structured, repetitive tasks with predictable inputs, such as invoice processing, payroll, and data entry across legacy systems. It excels at fast, consistent execution without requiring reasoning.
Agentic AI addresses the gaps RPA cannot fill. Agents can interpret unstructured data, adapt to change, and manage complex workflows that involve judgment, exceptions, and coordination across systems.
The optimal approach combines both. Use RPA for stable execution steps and agentic AI to orchestrate workflows, handle exceptions, and make decisions. Start by auditing processes to identify where rigidity causes friction, then apply RPA to deterministic segments and agentic AI to adaptive ones.
Begin with a small, measurable use case, prove value, and scale with governance in place. The goal is sustainable automation, not a fragile collection of bots.
The right architecture depends on your specific workflows, risk tolerance, and compliance requirements. Our healthtech engineers can assess your processes and recommend the model that actually fits.
👉Book a strategy call