Look, we’ve moved past the era where EHR compliance was just a tedious legal hurdle to clear before a product launch.
In 2026, if you’re scaling a digital health platform, compliance is the architecture. It’s the very thing that determines whether your system thrives as a global data engine or dies in a regulatory silo.
As healthtech organizations push into new markets, you’re hitting a “regulatory triad” that can stall even the most robust engineering roadmaps.
Global EHR expansion in 2026 depends on navigating the “regulatory triad” of HIPAA, GDPR, and Asian PDPL by transitioning from centralized storage to regionalized hybrid architectures.
Fragmented regulations across the US, Europe, and Asia create significant EHR compliance challenges. As a result, compliance is no longer a legal checkbox, but a core architectural requirement that defines scalability, market access, and business value.
If you’re a tech leader looking to expand, you know that “standardizing” your stack isn’t enough anymore. You need to build for flexibility.
In this guide, we’ll be breaking down how to navigate these conflicting requirements without rebuilding your infrastructure from scratch every time we enter a new country.
Also, we want to share key insights into global healthcare data compliance, clarify the requirements of HIPAA, GDPR, and PDPL, and provide guidance for healthcare organizations expanding their EHR platforms across the United States, Europe, and Asia.
Key takeaways
- Global EHR platforms must be designed for regulatory diversity, not regulatory convergence.
- HIPAA, GDPR, and Asian PDPL reflect fundamentally different philosophies, not just different rules.
- Data mobility strategies – SCCs, localization, or hybrid models are now board-level architecture decisions
Why EHR compliance is the new bottleneck for global scalability
The rise of cross-border healthcare data
EHRs have evolved into a constantly moving stream.
The numbers from 2025 tell a clear story: cross-border healthcare isn’t a niche experiment anymore; it’s a €465 million economy – according to the Cross-Border Healthcare Trend Report (2025). Patients are no longer tethered to local clinics, and specialized care is increasingly distributed across continents.
As a tech leader, you know that in this environment, data liquidity is your most valuable asset. But here’s the reality: you cannot have data liquidity without regulatory parity.
In the early days of healthtech, we built for the market we knew. But as we scale into 2026, the “move fast and break things” era has been replaced by the “move fast and stay compliant” mandate.
We need to stop viewing EHR compliance as a defensive “legal tax” and start seeing it for what it actually is: the ultimate scaling lever.
AI regulation and data interoperability
The “regulatory triad” isn’t just about where data sits; it’s about the provenance of the intelligence you’re building on top of it.
Historically, healthcare industry had a “grab and go” relationship with data.
As long as we could aggregate enough records into a training environment, the origin and specific consent context were often treated as secondary concerns.
Now is not the era of “black box” training. And that technical debt is coming due.
Under the AI Act in Europe and similar updates to Asian PDPLs (like Vietnam’s 2026 mandate), “data provenance” has moved from a data science theory to a hard legal requirement.
We are now in the age of Data Lineage Enforcement.
Today, healthcare organizations must be able to demonstrate transparent, legally valid data lineage and consent before any dataset can be used for model training or inference.
If you’re a CTO or Product Head, this is the scenario that should keep you up:
An AI diagnostic tool you’re ready to deploy globally today was trained on datasets from 2024. If those original datasets violated the strict localization or cross-border transfer rules of the time, the entire model is now potentially non-compliant or even illegal, regardless of current operational safeguards.
The fragmentation of privacy laws
Right now, the global landscape is split into three competing worldviews:
- HIPAA (US): Data protection as an operational safeguard, optimize control, reduce liability, protect providers.
- GDPR (EU): Data protection as a fundamental human right, patients own their data, platforms must yield control.
- Asian PDPLs: Data protection as digital sovereignty, data flow is conditional, localization and state oversight come first.
To scale effectively, we have to stop treating EHR compliance as a technical patch and start understanding the cultural DNA of the markets we’re entering.
Epic Systems with MyChart learned this the hard way. They built a powerhouse based on the HIPAA model: closed, provider-centric, and optimized for US workflows. As Epic and its peers move into Asia, the conflict escalates again. This time, from who owns the data to who controls the data economy itself.
The demand for patient-owned data forced a massive, painful shift toward open FHIR-based interoperability.
 Mapping the global healthcare data compliance landscape: three pillars
Mapping the global healthcare data compliance landscape: three pillars
1. HIPAA (The United States): rigidity in infrastructure
HIPAA remains the bedrock of US healthcare, but in 2026, the focus has transitioned to interoperability security.
- Core philosophy: HIPAA protects patient privacy, secures health information, limits use to the minimum necessary, and allows appropriate sharing for healthcare operations.
- Technical requirements: adopt NIST-aligned security controls, including strong encryption, robust access management, and well-governed Business Associate Agreements (BAAs) across all third-party integrations.
- The critical leadership risk: Most healthcare organizations are compliant on paper. The real risk emerges in daily operations, where cloud deployments, APIs, and partner integrations change faster than policies can keep up.
The gap between governance and execution is where compliance failures occur often without leadership visibility. Closing that gap requires continuous oversight, not periodic audits.
2. GDPR (The European Union): the philosophy of consent
With the European Health Data Space (EHDS), GDPR remains the foundation, but healthcare in 2026 places greater emphasis on patient control and data sharing across an open, interoperable ecosystem.
- Core philosophy: Patients are the primary rights-holders, while organizations act as trusted custodians of health data. Systems must enable strong individual control within GDPR’s legal framework.
- Technical requirements: Implement granular consent management that clearly separates treatment, research, and secondary data use. Systems should support data portability and interoperability standards, such as HL7 FHIR, to enable seamless EHR exchange.
- The critical leadership risk: Legacy consent is a growing threat. Reusing outdated consent for AI and machine-learning initiatives can invalidate R&D outcomes if the original consent did not explicitly cover advanced data processing.
3. PDPL (Asian): sovereignty & variety
Asia in 2026 views healthcare data as a national security asset rather than a private commodity.
- Core philosophy: Personal health data must be protected from foreign access and aligned with national security and public interest priorities. Cross-border data access is permitted, but tightly regulated rather than assumed by default.
- Technical requirements: Organizations must adopt multi-local architectures, ensuring sensitive EHR data remains within national borders. Cross-border use requires regulatory approval, strong anonymization, or privacy-preserving analytics at the source.
- Critical leadership risk: Compliance lag is a growing threat. Localization rules can change rapidly in response to geopolitical or security shifts, and reliance on a single global cloud strategy can trigger costly re-architecture when local requirements tighten.
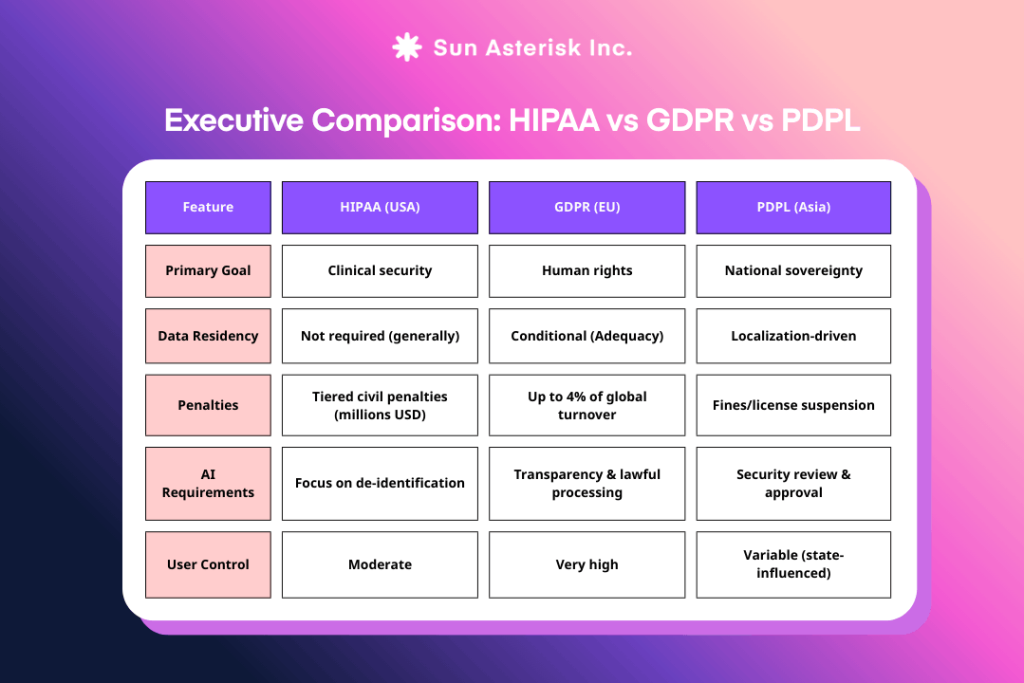
Executive global EHR compliance comparison: regulatory nuances for decision makers
 Global expansion strategy: mastering data mobility & residency
Global expansion strategy: mastering data mobility & residency
We’ve reached the point where EHR compliance must be programmable. If you can’t toggle data residency, automate your Transfer Impact Assessments (TIAs), or isolate PHI at the edge without breaking your global AI models, you aren’t scaling.
That’s when you’re just accumulating technical debt.
Here is how we’re bridging the gap between “data everywhere” and “data nowhere” through a modular, hybrid strategy.
1. Using Standard Contractual Clauses (SCCs) for global interoperability
When transferring data from the EU to countries without an adequacy decision, SCCs remain the primary legal mechanism enabling cross-border interoperability. Under GDPR, signing SCCs alone is no longer sufficient; organizations must conduct a Transfer Impact Assessment (TIA) to ensure local laws do not undermine the contractual protections
By 2026, leading organizations are moving beyond static compliance toward automated enforcement models, where transfer risks are continuously monitored and data flows can be adjusted dynamically. While not mandated by GDPR, these approaches represent emerging best practices in compliance-by-design.
Failure to implement lawful and effective transfer mechanisms has been a recurring factor in major GDPR enforcement actions, with potential penalties reaching up to 4% of global annual turnover.
2. Managing data localization requirements
- Localize sensitive patient data by design: Keep raw EHR/EMR and identity data within jurisdictional boundaries to meet HIPAA safeguards, GDPR consent obligations, and PDPL residency mandates.
- Separate data residency from analytics and AI: Process identifiable data locally, while allowing de-identified, policy-approved datasets to power global analytics and AI without violating cross-border rules.
- Build for regulatory change, not regulatory stability: Use modular, hybrid architectures that can adapt quickly as localization and transfer laws evolve across the US, Europe, and Asia.
3. Hybrid architecture for compliance & performance
To balance the two extremes: strict local compliance and global operational performance, healthcare organizations in 2026 no longer view compliance as a constraint, but as an architectural advantage.
- HIPAA (United States): Security at the Core
Sensitive PHI is processed within tightly controlled service boundaries, enforcing least-privilege access, auditability, and breach containment. Centralized governance ensures continuous security oversight as systems scale. - GDPR (Europe): Consent-Driven Data Mobility
Patient-identifiable data remains under strict consent and purpose controls. Only approved, de-identified datasets move into global analytics environments, preserving interoperability while respecting individual rights. - PDPL (Asia): Sovereignty by Design
Raw health data stays in-country by default. Local processing zones satisfy residency mandates, while only policy-approved outputs participate in cross-border workflows.
According to Amazon Web Services, the hybrid approach combines AWS-managed and customer-managed infrastructure under a single operational view, using consistent AWS services to deploy and manage workloads.
Sun* partners with healthtech teams to build and operate EHR and EMR platforms on AWS – enabling secure data storage, AI-driven diagnostics, and scalable architectures designed to meet HIPAA, GDPR, and PDPL compliance requirements.
Let Sun* turn EHR compliance into your global growth advantage
As we look at the landscape in 2026, what was once a legal obligation is now a design principle, with compliance defining an organization’s ability to scale, enter new markets, and sustain long-term value.
Don’t let your global expansion stall due to “legacy consent” or localization hurdles. Let’s discuss how we can move your project from a successful pilot to a transformative global platform.