When we talk about the patient experience, we usually talk about empathy. But the real bottleneck is connectivity. By moving toward agentic AI in healthcare — specifically through Multi-Agent Orchestration — we can finally stop asking patients to act as their own data integrators.
It’s about shifting the burden from the person to the architecture.
Behind every clinical encounter, lab result, and treatment decision sits a fragmented ecosystem of systems, data spread across EHRs, laboratories, imaging platforms, and claims databases.
Each system is optimized for its own workflow, but few are designed to work together. And in the absence of true coordination, the patient is left to act as the integrator.
Until that changes, the patient experience can only improve at the margins; it cannot fundamentally evolve.
This is the patient experience problem we rarely acknowledge.
Key summary
- Multi-Agent Orchestration (MAO) creates an intelligent layer over legacy silos
- It uses the Model Context Protocol (MCP) to bridge HL7, SQL, and FHIR
- “Agent-Critic” loops ensure HIPAA compliance and clinical safety
Why EHR fragmentation still persists in 2026
If you’re wondering why we’re still talking about fragmentation in 2026, it’s because we aren’t just fighting a technical battle, we’re fighting a legacy of “digital silos.”
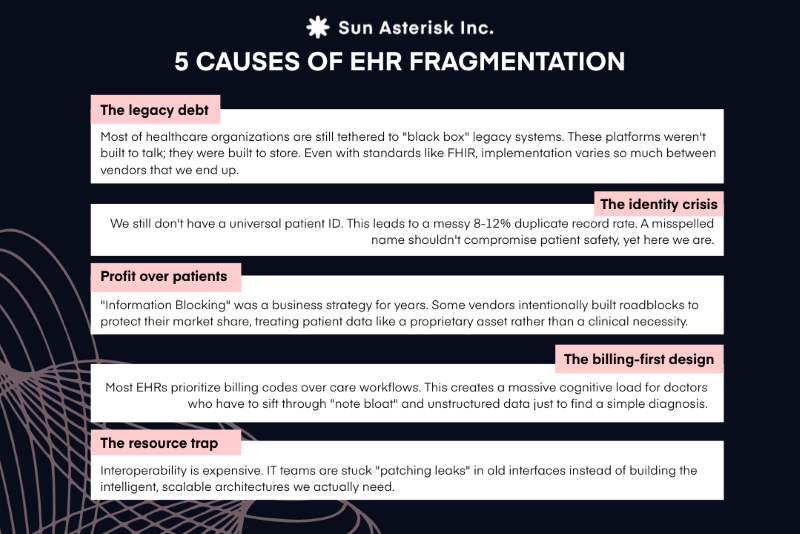
- The legacy debt: Over 55% of healthcare organizations are still tethered to “black box” legacy systems. These platforms weren’t built to talk; they were built to store. Even with standards like FHIR, implementation varies so much between vendors that we end up with “interface discrepancies” that garble the data.
- The identity crisis: We still don’t have a universal patient ID. This leads to a messy 8-12% duplicate record rate. A misspelled name shouldn’t compromise patient safety, yet here we are.
- Profit over patients: “Information Blocking” was a business strategy for years. Some vendors intentionally built roadblocks to protect their market share, treating patient data like a proprietary asset rather than a clinical necessity.
- The billing-first design: Most EHRs were designed by accountants, not clinicians. They prioritize billing codes over care workflows. This creates a massive cognitive load for doctors who have to sift through “note bloat” and unstructured data just to find a simple diagnosis.
- The resource trap: Interoperability is expensive. Between tight budgets and the fact that 58% of systems are understaffed, IT teams are stuck “patching leaks” in old interfaces instead of building the intelligent, scalable architectures we actually need.
Multi-Agent Orchestration (MAO) represents a fundamental shift in architectural thinking. Rather than dismantling existing data silos, MAO introduces an intelligent orchestration layer on top of them.
We’re shifting the goalpost from basic data exchange to true AI interoperability, where the data isn’t just moved, but understood and acted upon by the orchestration layer.
By deploying a network of specialized AI agents, organizations can seamlessly access legacy systems, resolve patient identity and record duplication, and transform raw clinical data into actionable intelligence, dramatically reducing manual cognitive load for clinicians while unlocking scalable, patient-centered care.
So, what is Multi-Agent Orchestration in healthcare?
Multi-agent orchestration refers to the coordinated collaboration of multiple AI agents working toward a shared clinical or operational objective within a structured, outcome-driven healthcare system.
It represents the next frontier of agentic AI in healthcare. It moves us from passive models that answer questions to active systems that execute clinical workflows.
Instead of operating in isolation, these agents continuously communicate, share clinical context, and collaborate to manage complex, cross-system workflows, such as care coordination, clinical documentation, and utilization management, more effectively.
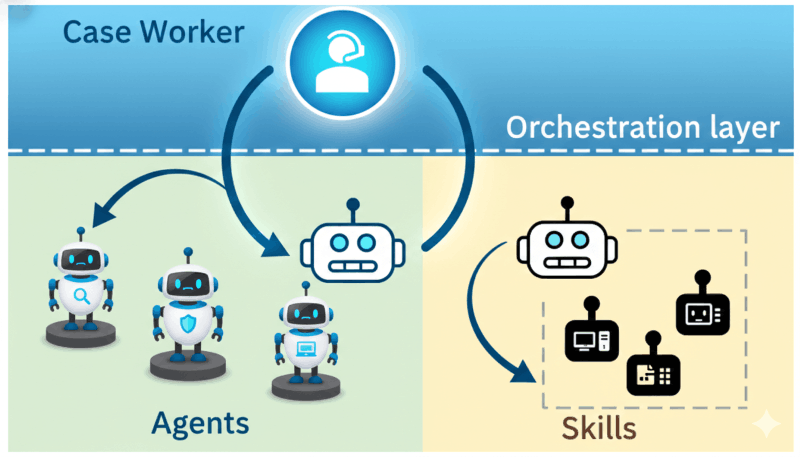
Let’s go a bit further down into the technical definition. The core components of MAO in healthcare include:
- AI agents: Specialized, task-focused agents designed to support clinical and administrative functions, such as interpreting clinical data, summarizing patient histories, validating documentation for compliance, or assisting with care coordination.
- Orchestration system: The coordination layer that governs agent behavior, assigns tasks based on clinical context and workflow state, monitors execution, and enforces safety, compliance, and accountability.
- Communication methodology: Standardized, reliable mechanisms for exchanging clinical context, decisions, and signals between agents while maintaining data integrity and regulatory compliance.
- Clinical knowledge base: A shared, longitudinal repository containing patient data, clinical guidelines, workflows, policies, and historical context, enabling agents to reason consistently, stay aligned with standards of care, and support accurate clinical decision-making.
4 common Multi-Agent Orchestration patterns
Across multiple healthcare AI deployments, we have observed that successful agentic systems rarely follow a single orchestration model.
Instead, these patterns emerge organically as teams confront real-world constraints: fragmented EHRs, inconsistent data quality, strict governance requirements, and unpredictable clinical workflows.
Our experience with the inherent messiness of healthcare environments has highlighted a key challenge: developing orchestration patterns that balance rigid regulatory control with operational adaptability.
The following models represent the most common approaches we’ve seen in practice, each optimized for different operational and clinical realities.
1. Hierarchical orchestration
A Manager Agent receives requests from users and decomposes them into smaller tasks, which are then delegated to specialized Worker Agents, such as an agent focused on medication history or another dedicated to lab results. The Manager Agent aggregates the outputs and delivers a consolidated response.
2. Centralized orchestration
A central Orchestrator maintains control over the entire workflow. This model is particularly effective for enforcing healthcare compliance and security requirements, as every agent action is closely monitored and governed.
3. Adaptive orchestration
This represents the highest level of flexibility. The system dynamically adjusts workflows based on real-time context.
For example, if data from one EHR system becomes unavailable or unreliable, the orchestrating agent can automatically reroute queries to a fallback system or modify its retrieval strategy without manual intervention.
4. Emergent orchestration
Agents interact and collaborate autonomously without relying on rigid, predefined scripts. While this approach is harder to govern, it is critical for addressing rare clinical cases or highly chaotic data environments where hard-coded workflows inevitably break down.
Examples of Multi-Agent Orchestration
Molecular Tumor Boards
Microsoft developed the Healthcare Agent Orchestrator (HAO), which integrates natively into Microsoft Teams. In tests on the “TB-Bench” dataset consisting of 71 real oncology patients, HAO’s “Patient History” agent successfully captured 94% of high-importance clinical facts. It parses clinical notes, pathology reports, and imaging data to create a comprehensive, citation-backed timeline for oncologists.
Clinical Trial Matching (TrialGPT)
This system uses a trio of agents: Retrieval, Matching, and Ranking, to determine if a patient is eligible for specific clinical trials. In practice, TrialGPT accurately screened out 94% of ineligible trials, evaluated criteria with 87.3% accuracy, and allowed human doctors to complete trial screening tasks 42.6% faster.
How does Multi-Agent Orchestration actually work to solve EHR fragmentation?
Look, we all know EHR integration is usually where good code goes to die. But instead of building another brittle ETL pipeline, we’ve been leaning into Multi-Agent Orchestration (MAO). It’s less about “linking” data and more about treating fragmented silos as one big, coherent conversation.
Here’s the breakdown of how we’re actually shipping this:
The manager-worker hierarchy
Standard API calls are too blunt for healthcare. If a doc asks for an oncology summary, you can’t just dump a 200-page PDF.
We use a Manager Agent to decompose that high-level ask into surgical sub-tasks. This isn’t just a basic prompt; it’s a sophisticated approach to LLM orchestration for EHR data, where a Manager Agent handles the heavy lifting of task decomposition.
The retrieval layer of MCP & protocol translators
The “monolithic integration” dream is dead.
We’re now using Fetcher Agents as smart wrappers. By leveraging the Model Context Protocol (MCP), these agents act as our universal translators.
Our MCP implementation allows us to treat disparate EHRs like a standardized “Secure USB Port” for AI, enforcing read-only policies without the integration nightmare.
We’ve got one agent speaking FHIR, another querying SQL, and a third scraping legacy XML.
The best part? We aren’t writing custom glue code for every new endpoint anymore; we’re just deploying a new agent to bridge the gap.
On-the-fly context assembly – the dynamic RAG
Retrieval Augmented Generation (RAG) is the secret sauce here. The agents don’t just “find” a file; they assemble it. They’re pulling fragmented attributes—like tumor biomarkers buried in unstructured notes—and normalizing them into a Virtual Unified Record in real-time. It’s essentially solving a moving puzzle where the pieces are scattered across three different hospitals.
The agent-critic safety loop
The biggest pushback we get is (rightly) about hallucinations or conflicting data—like a med list that doesn’t match an allergy log.
We handle this with an agent-critic workflow.
Before anything hits the UI, a critic agent cross-verifies the output for logical consistency and HIPAA compliance. If two sources disagree, the system triggers a logic check before the doctor ever sees a screen.
What healthtech leaders are saying about Multi-Agent Orchestration
Talking to other teams in this space, the vibe is pretty unanimous: we’re officially over the ‘chatbot’ era.
Nobody wants another glorified search bar. Here’s what’s actually on the roadmap for folks building at the edge:
From “Chatting” to “Solving”
Hitul Mistry, writing for the Digiqt Blog on Healthcare Supply Chain, highlights that AI agents are fundamentally better than traditional automation because they are “goal-oriented” and “exception smart”.
Instead of just raising IT tickets, agents diagnose root causes and propose remedies. He predicts that the future of healthcare logistics lies in “connected multi-agent ecosystems” that simulate and execute supply flows across global routes while maintaining strict compliance.
Clinical safety is the #1 concern
While optimism is high, some researchers like Zhu and partners caution about the computational and mental costs of Multi-Agent Systems.
They note that for certain structured prediction tasks, single-LLM systems can sometimes perform just as well, meaning developers must ensure that the complexity of an agentic system is justified by the demands of the clinical environment.
We’re seeing massive ROI in specific, high-complexity areas:
- Oncology: Automated preparation for Molecular Tumor Boards, where agents synthesize history, imaging, and pathology in minutes.
- Supply Chain: Using “signal-monitoring” agents to predict cold-chain failures or stock-outs before they happen.
- Triage: Improving accuracy in overcrowded ERs by simulating a multi-specialty team (Nurse, Physician, Pharmacist agents) for every patient.
- Standardization via MCP: Technical leaders are rallying around the Model Context Protocol (MCP). Think of it as a “Secure USB Port” for AI. It allows us to plug agents into proprietary EHRs safely, enforcing strict HIPAA read-only policies without the nightmare of custom-coding every integration.
The rise of the “AI hospital” simulation
The most forward-thinking leaders are already looking at “Agent hospitals”, simulated environments where AI doctors and nurses “practice” on virtual patients to reach 90%+ diagnostic accuracy before they ever touch a real-world workflow.
What comes next: from interoperability to intelligent orchestration
The next leap forward in healthcare isn’t simply about connecting systems; it’s about enabling data to be intelligent enough to organize itself.
AI can now reconcile, normalize, and contextualize fragmented data across disparate sources, creating an AI-ready foundation that transforms disconnected records into a continuously learning ecosystem. In this model, patients are no longer forced to act as the integrators of their own care, on top of everything else they already manage.
This shift, from interoperability to intelligence, requires more than a single model or dashboard. It demands a new architectural layer capable of coordinating how data is understood, reasoned over, and acted upon across systems.
This is where Multi-Agent Orchestration enters the picture.
Rather than treating AI as a point solution, Multi-Agent Orchestration introduces a network of specialized agents, each responsible for a specific clinical or operational context, working together under an intelligent coordination layer.
It is this orchestration that allows healthcare systems to move from simply exchanging data to delivering coordinated, context-aware care at scale.
EHR fragmentation is a legacy problem, but it requires a future-forward solution. Multi-Agent Orchestration provides the flexibility and intelligence needed to turn a mess of data into a masterpiece of clinical insight.
Is your organization ready to move beyond silos?
Contact our engineering team today for a tech deep-dive on how Multi-Agent Orchestration can unify your clinical workflows.