In the landscape of healthcare IT outsourcing, choosing to build or buy is a long-term commitment to a cost structure that will govern your technology organization’s potential for the next five years.”
Run the complete analysis: full lifecycle scope, loaded cost rates, maintenance multipliers, and opportunity cost. In most scenarios, a well-governed healthcare IT outsourcing partnership will deliver more clinical and operational value per dollar than an internal build, not because vendors are inherently superior, but because specialization compounds.
A vendor whose entire business depends on maintaining and improving a clinical platform will always outpace an internal team managing a platform alongside ten other competing priorities.
In this article, we will explain this framework clearly and provide strategies for IT leaders to address the hidden costs of healthcare IT outsourcing.
Key takeaway
- The “Build” model often fails because it underestimates the “Maintenance” phase, which typically accounts for 60-80% of total lifecycle costs.
- Healthcare IT is unique due to the constant evolution of clinical guidelines and regulatory requirements.
- The true cost of outsourcing must be measured against the opportunity cost of diverting internal talent from core patient-care innovations.
Why is “Build vs Buy” a misleading framework in healthcare IT outsourcing?
The build-or-buy heuristic has been a reliable shortcut for technology decisions for decades. The logic is clean: compare the cost to build something in-house against the cost of healthcare IT outsourcing or licensing from a vendor, factor in strategic fit, and decide. For manufacturing equipment, fleet vehicles, or even general business software, this math is solid.
But the traditional framework was designed for a world where assets depreciate on a predictable curve where a forklift bought today is essentially the same forklift three years from now, just older. Healthcare software doesn’t work that way.
In the standard model, the build decision is treated as a discrete event. In the reality of healthcare IT outsourcing, however, it’s the start of an open-ended operating expense. The moment you ship, the clock starts on your next major update, not because you chose to improve, but because your clinical, regulatory, and competitive environment demands it.
The framework that actually reflects this reality looks different:
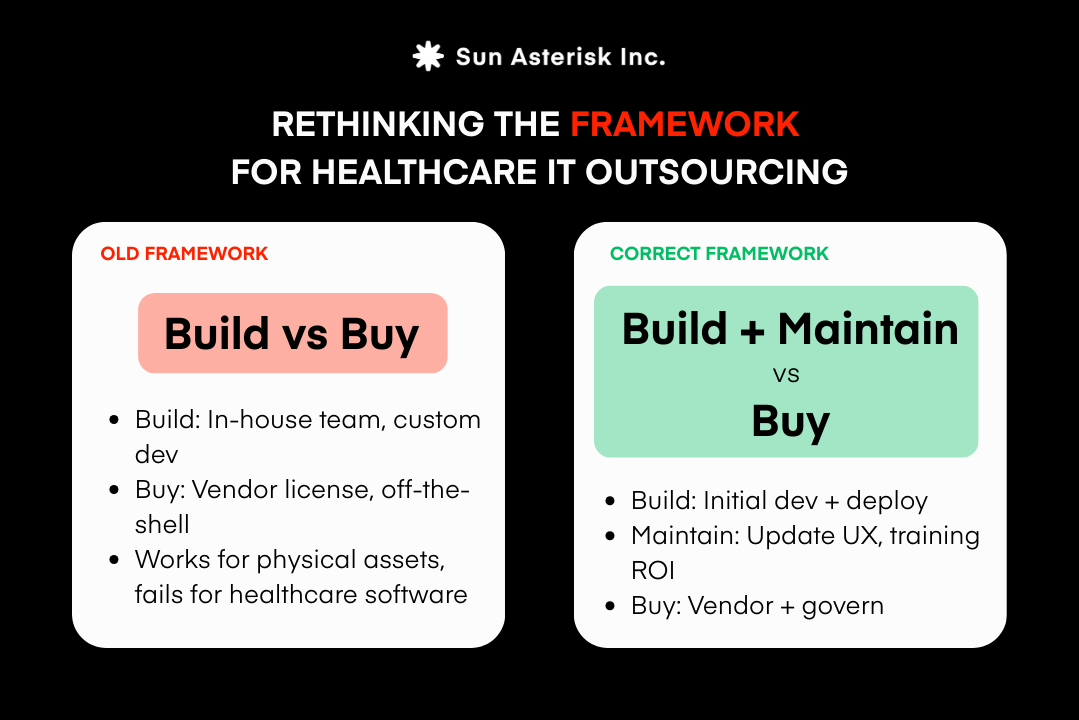
Once you make this shift, the hidden costs become visible, and the decision becomes far more nuanced than a simple line comparison between development quotes and vendor pricing.
The Hidden Iceberg: Why “Maintenance” Costs So Much in Healthcare IT Outsourcing?
Most “build” business cases are built around one moment in time: go-live. The cost model captures development sprints, infrastructure setup, initial integrations, and a first round of training.
It looks complete. What it almost never captures is everything that begins the day after launch and doesn’t stop for as long as the system is running.
In our experience supporting health systems through both build and healthcare IT outsourcing decisions, ongoing maintenance consistently accounts for the majority of the total five-year software cost.
Not because organizations planned poorly, but because the nature of healthcare software makes maintenance structurally expensive in ways that general enterprise IT is not.
There are five reasons why, and understanding each one is essential before any honest comparison between building in-house and outsourcing healthcare IT can be made.
1. Clinical Content & Algorithm Updates in Healthcare It Outsourcing
Clinical software is only as good as the clinical knowledge inside it. Care pathways, risk-scoring models, diagnostic algorithms, and decision-support logic are all built on evidence and evidence moves. Professional societies update treatment guidelines. Regulatory bodies revise quality measures.
New drug approvals change first-line therapy recommendations. A sepsis detection algorithm validated in 2025 may need to be retrained and revalidated by 2026 as the underlying patient population data shifts.
Each of these updates is not a simple content edit. In a regulated healthcare environment, every change to clinical logic requires a validation cycle: clinical review, QA testing, sign-off from your compliance or medical affairs team, and a controlled deployment.
If your platform surfaces recommendations to clinicians at the point of care, you also carry liability exposure for content that is out of date.
Clinical content maintenance is not a background task. It requires dedicated clinical informatics resources – people who sit at the intersection of medicine and technology and a formal governance process.
In a purpose-built outsourced platform, this infrastructure already exists. In an internal build, you are constructing it from scratch and funding it indefinitely.
2. Feature Development & Product Relevance
There is a version of every internal build story that goes like this: the system launches, it works, clinicians adopt it, and then slowly, quietly – it starts to fall behind. Not because anything broke, but because everything around it kept moving.
Healthcare IT does not have a stable finish line. Interoperability standards evolve, the shift to HL7 FHIR APIs, for instance, has required substantial re-engineering across virtually every clinical platform built before 2020.
Patient engagement expectations, shaped by consumer technology, continue to rise. AI-assisted documentation, ambient clinical intelligence, and real-time analytics are moving from differentiators to baseline expectations faster than most internal roadmaps can accommodate.
Sustaining product relevance requires something most internal IT teams are not structured to provide: a dedicated product function.
Not just engineers who fix bugs, but product managers who track the competitive and regulatory landscape, designers who run continuous user research, and engineering capacity reserved specifically for new capability, not consumed entirely by maintenance and compliance work.
3. UI/UX Continuous Improvement
Poor usability in clinical software is not a minor inconvenience. It is a documented driver of clinician burnout, reduced adoption, workaround behaviors that introduce patient safety risk, and ultimately, system replacement.
The American Medical Association and multiple health system studies have identified interface design as one of the primary contributors to physician dissatisfaction with clinical technology.
What makes this particularly challenging from a maintenance perspective is that usability is not a problem you solve once. It is a discipline you sustain.
User needs evolve as workflows change. New staff arrive with different mental models and digital expectations. Features that worked intuitively for one generation of users create friction for the next.
The only way to stay ahead of this is through continuous user research, design iteration, and usability testing, none of which are one-time costs.
In an outsourced platform with a large user base, UX investment is distributed across many clients and driven by aggregated usage data at a scale no single health system can match internally.
In a proprietary build, every UX improvement is funded entirely by your organization – and in most cases, it competes with compliance work and feature development for the same limited engineering and design resources.
4. Staff Training & Change Management
Healthcare software updates don’t announce themselves and get absorbed passively the way a smartphone app update might. In clinical environments, every meaningful change to a system that touches patient care requires structured, validated training: role-specific, documented, and delivered in a way that doesn’t disrupt care delivery.
This creates a training obligation that is tied not just to software releases, but to staff turnover, which in healthcare runs significantly higher than most other industries. New nurses, physicians, and administrative staff joining your organization need to be trained on your systems, regardless of whether anything changed.
Every workflow modification, every new module, every integration with a new device or data source triggers a fresh training cycle for the affected population.
The cost of this is rarely modeled honestly in build proposals. It includes curriculum development and maintenance, scheduling and logistics across clinical departments, competency assessment, and documentation for accreditation purposes. And the cost of protected time – pulling clinical staff away from patient care to sit in training.
For health organizations considering a build, a realistic training and change management budget for a single clinical platform over five years will frequently surprise leadership when it is finally calculated in full.
5. Outcomes Monitoring & ROI Assessment
A clinical platform that cannot demonstrate its impact on patient outcomes and operational performance will eventually lose its budget justification, particularly as health systems face increasing pressure from value-based care contracts, CMS quality reporting requirements, and board-level scrutiny of technology ROI.
Outcomes monitoring is not simply running a dashboard.
It requires a measurement framework: clearly defined clinical and financial metrics, data pipelines that connect the platform to your analytics infrastructure, and attribution logic that isolates the platform’s contribution from other variables. And reporting cadences that give leadership the visibility they need to make resourcing decisions.
Building and maintaining this infrastructure is a non-trivial investment, and it needs to be refreshed as your quality program evolves, as payer contracts change, and as the platform itself adds new capabilities.
In a mature outsourcing partnership, outcome accountability can be embedded contractually. Vendors with skin in the game have a strong incentive to build measurement into the product and report on it proactively.
In an internal build, the entire measurement burden falls on your analytics and clinical quality teams – quietly, permanently, and almost always without a dedicated budget line.
Healthcare IT Outsourcing: A Practical Framework to Calculate the True Cost
The goal of this framework is not to bias the outcome toward outsourcing; it’s to ensure both options are evaluated on equal, honest terms.
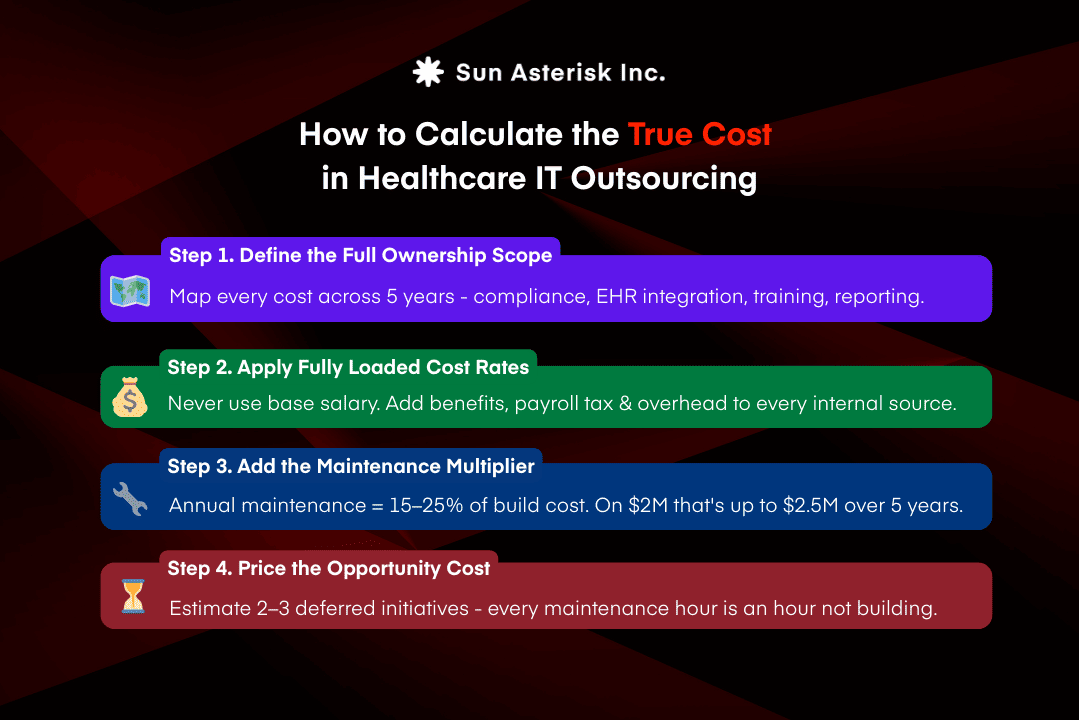
Step 1. Define Ownership Scope for the Full Lifecycle
Refuse to open a spreadsheet until you have mapped every function your system must perform over five years, not just at go-live. Include: initial development or implementation, HIPAA and ONC compliance updates, clinical content versioning, infrastructure scaling, security patching, EHR integration maintenance, and outcomes reporting all belong in the scope before a single dollar figure enters the model.
If your build estimate doesn’t include a line item for clinical content governance, you haven’t scoped the build; you’ve scoped the launch. Apply the same discipline to healthcare IT outsourcing proposals: confirm which functions are included in the contract, which are shared, and which remain entirely yours.
Step 2. Apply Fully Loaded Internal Cost Rates
For example, a healthcare software engineer with a $125,000 base salary typically costs $185,000–$210,000 annually once benefits, payroll taxes, management overhead, and workspace are factored in. That 50–70% gap above base salary applies to every internal resource in your model – engineers, clinical informatics specialists, QA analysts, trainers, and project managers.
Critically, apply these rates to your ongoing maintenance team too because that team doesn’t disappear after go-live. In a healthcare IT outsourcing engagement, these costs are distributed across the vendor’s client base. In an internal build, they sit on your payroll every year, for as long as the system runs.
Step 3. Apply the Maintenance Multiplier
Before any vendor pricing enters the comparison, one number must already be in the build column: the five-year maintenance floor.
We have made preliminary estimates for the hypothetical model. Annual maintenance for healthcare software consistently runs 15–25% of the original build cost per year. On a $2 million build, that is $300,000–$500,000 annually, just to keep the system current and compliant, before any new features are developed. Over five years, that floor adds $1.5–$2.5 million to the build column. A $2 million investment becomes a $3.5–$4.5 million commitment before the organization has spent a dollar on growth.
This is the figure most missing from build analyses that conclude building is cheaper than healthcare IT outsourcing. It is the predictable, structural cost of owning software in a regulated clinical environment.
Step 4. Price the Opportunity Cost
Every engineer hour spent on compliance updates, integration maintenance, and clinical content revisions is an hour not spent building what only your organization can build – the predictive analytics model, the patient engagement tool, the operational dashboard your CMO has been requesting for two years.
Opportunity cost is difficult to quantify but too consequential to omit.
A practical approach: estimate the value of two or three deferred strategic initiatives over five years and include that figure as a range in the build column. When teams do this honestly, it frequently shifts the comparison more than any other single variable. Because it makes visible what the build decision is actually trading away, and what a well-scoped healthcare IT outsourcing partnership frees your team to pursue instead.
Before you commit to either path, our team will sit down with you to run the real numbers: full TCO analysis, maintenance projections, and an honest assessment of whether building or buying serves your clinical and operational goals better.
Let’s figure out the right path together. Talk to our healthtech experts