Healthcare data interoperability is one of the biggest barriers to turning patient data into real clinical and operational insight. We see healthcare leaders struggle with fragmented, provider-centric EHRs that limit longitudinal visibility, slow decision-making, and constrain population health and research.
In this article, we share how you can approach healthcare data interoperability at scale, combining interoperable architectures, governance, and policy alignment to enable secure data exchange while meeting regulatory demands.
Key takeaway:
Fragmented data costs healthcare organizations more than money, it costs time, accuracy, and patient trust. The path forward requires more than connecting systems: it demands aligned leadership, shared standards, and a long-term commitment to treating interoperability as a core business capability.
What is Healthcare Data Interoperability?
Data Interoperability in healthcare is the ability of health information systems like Electronic Health Records (EHRs), lab systems, and imaging software, to exchange, interpret and reuse data unambiguously.
It is not merely a technical connection but a multifaceted framework designed to ensure that clinical meaning is preserved across different care settings, technologies, and organizations.
True interoperability goes beyond simple data exchange. It ensures that information shared between systems is:
- Structured and standardized
- Clinically meaningful
- Timely and accurate
- Usable within existing workflows
Effective interoperability functions across 04 three distinct levels:
- Foundational: The basic exchange of raw data from one system to another without requiring the receiving system to interpret it.
- Structural: The exchange of data where the format or structure is preserved, such as message format standards like HL7 FHIR, allowing the receiving system to interpret the data field.
- Semantic: This level enables the exchange and reuse of data where the meaning is interpreted and preserved, and ensures that clinical knowledge is controlled, shareable, and reusable for decision support and analytics.
- Organizational: The highest level, aligns policies, governance, workflows, legal agreements, and incentives across organizations so data exchange can occur at scale and be sustained. This includes data governance models, consent management, trust frameworks, and operational processes.
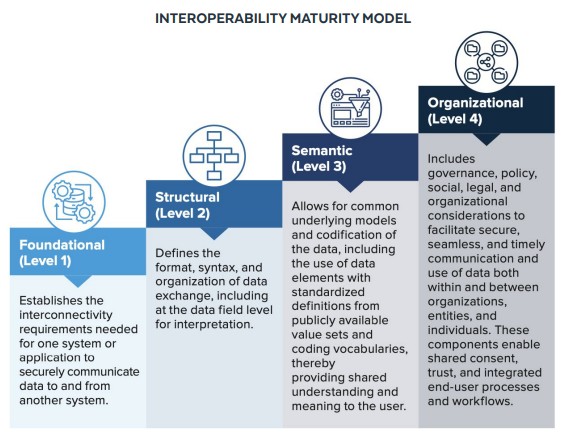
Interoperability maturity model (Source: Snowflake)
Why Improving Interoperability Matters in Healthcare Industry
In the US alone, it is estimated that nearly $30 billion is wasted annually due to poor data integration and the resulting duplication of medical tests. This financial drain is symptomatic of a fragmented system where a single patient’s health narrative is often scattered across dozens of incompatible digital silos.
- Clinical Accuracy: It eliminates “blind spots” by providing clinicians with a 360-degree view of a patient’s medical history, which is vital for preventing the 250,000+ deaths attributed to medical errors each year.
- Operational Resilience: It automates the exchange of information, replacing antiquated manual processes like faxing and manual data entry that lead to administrative burnout and delayed care.
- Patient Empowerment: It grants individuals true ownership of their health data, allowing them to transition between specialists or health systems without the burden of physically transporting paper records.
- Public Health Preparedness: It enables real-time reporting to health agencies, ensuring that emerging disease clusters are identified and contained before they become widespread crises.
What are the Biggest Barriers to Healthcare Data Interoperability?
Technical Fragmentation and Legacy Systems
- Legacy system fragmentation: Siloed legacy systems built on proprietary formats remain the primary technical barrier to interoperability, with 63% of implementations citing integration complexity as the main challenge.
- Uneven standards and semantics adoption: Despite the availability of modern standards such as HL7 FHIR, only 34% of organizations have achieved functional implementations, while inconsistent clinical terminologies (SNOMED CT, LOINC, RxNorm) continue to limit semantic interoperability.
The Challenge of “Semantic” Interoperability
- Prevalence of unstructured data: Nearly 80% of healthcare data remains unstructured (free-text clinical notes), significantly limiting its availability for real-time analysis, automation, and secondary use.
- Semantic loss during exchange: Most systems achieve only foundational or structural interoperability, preserving data transport but not meaning. Inconsistent terminology, vague clinical entries, and local abbreviations prevent reliable semantic interpretation, constraining clinical decision support and advanced analytics.
Information Blocking and Economic Barriers
- Information blocking as a systemic barrier: Many interoperability barriers stem from intentional business practices rather than technical limitations.
- Anti-competitive and restrictive practices: These include rent-seeking through excessive interoperability fees, restrictive contractual “gag clauses” that limit transparency, and refusal to license interoperability components, all of which hinder competition and slow ecosystem-wide innovation.
Workflow and Human Factors
Workflow-centric failure: Interoperability often fails at the point of care, with 74% of AI and data initiatives breaking down due to poor workflow integration and increased clinician documentation burden rather than technical limitations.
Privacy, Security, and Governance
Security-compliance trade-offs: Enabling patient access to third-party apps introduces security and governance risks, with providers facing complex information-blocking exceptions and unresolved data ownership and control issues, which remain barriers in nearly half of interoperability implementations.
Standards That Guide Healthcare Data Interoperability
HL7 (Health Level Seven)
HL7 (Health Level Seven) is an international standards organization that defines how healthcare data is structured, exchanged, and understood across different systems to enable interoperability.
Its standards operate at the application layer, focusing not just on data transport but on preserving clinical meaning. HL7 includes widely used messaging standards like HL7 v2, document standards such as CDA, and the modern, API-based FHIR standard designed for cloud, mobile, and scalable data exchange.
Together, these standards form the foundation for consistent, secure, and interoperable data sharing across EHRs, providers, payers, and third-party applications in the healthcare ecosystem.
FHIR (Fast Healthcare Interoperability Resources)
FHIR (Fast Healthcare Interoperability Resources) is a modern interoperability standard developed by HL7 to enable fast, flexible, and scalable exchange of healthcare data across systems.
It uses modular data units called resources (such as Patient, Observation, and Medication) and supports RESTful APIs, JSON, and XML, making it well-suited for cloud-native architectures, mobile applications, and third-party integrations.
By combining standardized data models with web technologies and strong security mechanisms, FHIR simplifies integration, improves semantic consistency, and accelerates the development of interoperable healthcare applications.

Other Key Players and Concepts
- OINC: For lab test standardization
- SNOMED CT: For clinical terminology
- ICD-10: For diagnosis coding
- APIs: The digital messengers that make real-time data exchange possible
Best Practices and Strategies for Healthcare Data Interoperability
To achieve effective healthcare data interoperability, organizations must move beyond simple connectivity to a comprehensive strategy that addresses technical structure, semantic meaning, regulatory compliance, and clinical workflow.
Why the Cloud is the Right Foundation?
The shift to cloud data platforms is not simply a technology upgrade.
It is a structural response to a problem that has plagued healthcare for decades: data that lives in silos, can’t talk to each other, and costs more to maintain than it delivers in value.
The most important advantage the cloud offers is not speed or storage – it’s decoupling. Cloud architectures allow compute and storage to scale independently, which means organizations pay for what they actually use, and can handle wildly variable workloads (a surge in analytics during a public health event, for example) without over-provisioning expensive on-premises infrastructure year-round.
Beyond cost, the cloud enables something that on-premises systems structurally cannot: real-time, cross-organizational data collaboration with healthcare-grade compliance built in.
SOC 2 and HIPAA conformance, consistent governance of PHI and PII, and always-on resilience are no longer custom-built features, they’re baseline expectations of mature cloud platforms.
One underappreciated benefit is native support for semi-structured data formats like HL7 FHIR. This reduces the ETL complexity that traditionally bogs down integration projects and, critically, preserves clinical context that gets lost in translation between systems.
For interoperability, that context is everything.
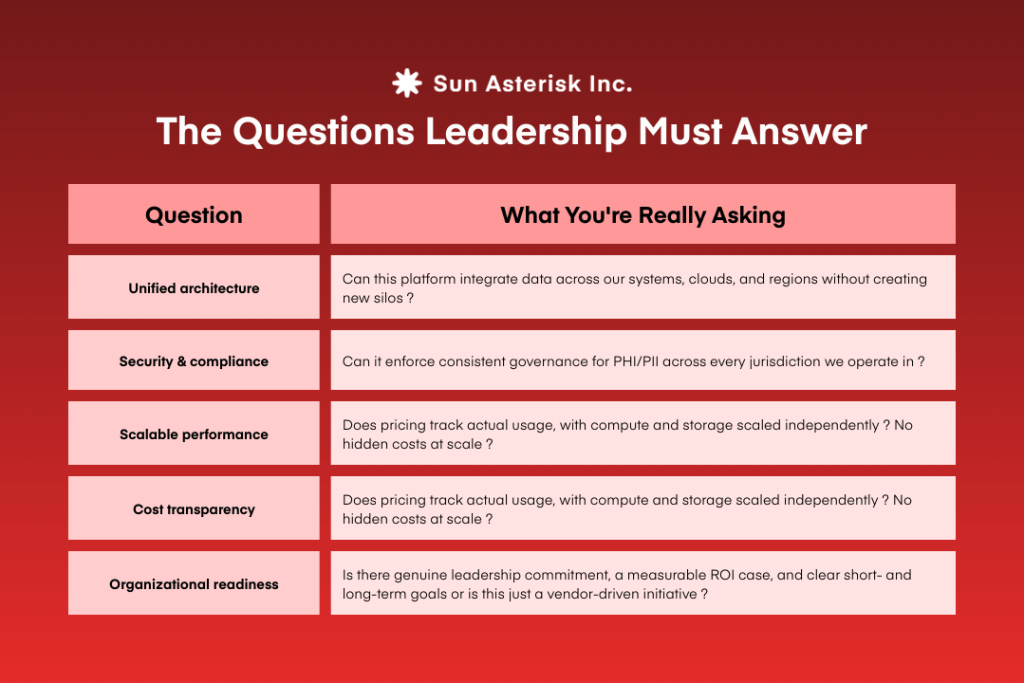
The Questions Leadership Must Answer
Before adopting any cloud strategy, decision-makers need honest answers to five questions. This is not a technical checklist, it is a strategic due diligence framework that should be reviewed at the executive level, not delegated entirely to IT.
Financial and Political Considerations: Who Needs to Care and Why
Technical teams can architect a perfect interoperability solution and still watch it fail because no one agrees on who owns the budget, who has authority over shared data, or what success actually looks like.
Interoperability projects fail most often not because the technology doesn’t work, but because the organizational conditions for success were never established.
A fragmented governance model, competing departmental priorities, or unclear funding accountability will stall execution regardless of what platform you’ve chosen.
The antidote is straightforward but requires discipline: define the strategy before selecting the tools, secure cross-functional buy-in that is tied to shared clinical and business outcomes (not just IT deliverables), and assign clear ownership over scope, timelines, and resources.
Change management is not a “soft” afterthought, it is a delivery-critical function. The people whose workflows will change need continuous communication and realistic expectations, or resistance compounds into delay.
A useful framing: treat interoperability as a business program that happens to have a technology component, not a technology project that happens to affect the business.
Establish a center of excellence
A Center of Excellence (CoE) is the organizational mechanism that prevents interoperability from being a one-time project and makes it a sustained capability.
The logic is simple: without a governing body, every initiative is a standalone effort with its own standards, its own politics, and its own definition of done.
What a CoE actually does is consolidate the lessons of all those standalone efforts into a repeatable model: shared standards, shared governance, shared tooling, and shared accountability.
It is also the entity that manages the ongoing tension between financial constraints, organizational politics, and technical ambition, a tension that does not resolve itself and requires active stewardship.
Crucially, a CoE should be use-case-driven, not standards-driven.
Starting from “what clinical or operational outcome are we trying to enable?” produces far more traction than starting from “what data standards should we adopt?” The former generates stakeholder energy; the latter generates committee meetings.
How Healthcare Organizations Achieve Data Interoperability
From our work with healthcare organizations, those who succeed with interoperability don’t treat it as a one-off integration effort. They build it as a long-term capability aligned with clinical and business outcomes.
They focus on:
- A clear interoperability roadmap tied to real clinical and operational goals
- Centralized, governed integration platforms instead of ad-hoc interfaces
- Early collaboration with vendors and ecosystem partners on shared data contracts
- Continuous monitoring of data quality, meaning, and downstream usability
Most importantly, interoperability is treated as a shared responsibility across IT, clinical leadership, compliance, and operations, turning data exchange into a foundation for scale, resilience, and AI readiness.
When interoperability works, healthcare organizations move faster, make better decisions, and deliver better outcomes. We help healthcare organizations design and implement interoperability strategies that go beyond technical integration.