The average clinic admin team spends around 13 hours per week on tasks that don’t require clinical judgment: insurance eligibility checks, prior authorization follow-ups, appointment reminders, intake form routing, or billing code verification.
These tasks are straightforward and necessary, and in theory, require minimal human intervention. Yet when clinics evaluate solutions, the conversation often centers on tools rather than outcomes—especially when it comes to understanding the true healthcare workflow automation cost.
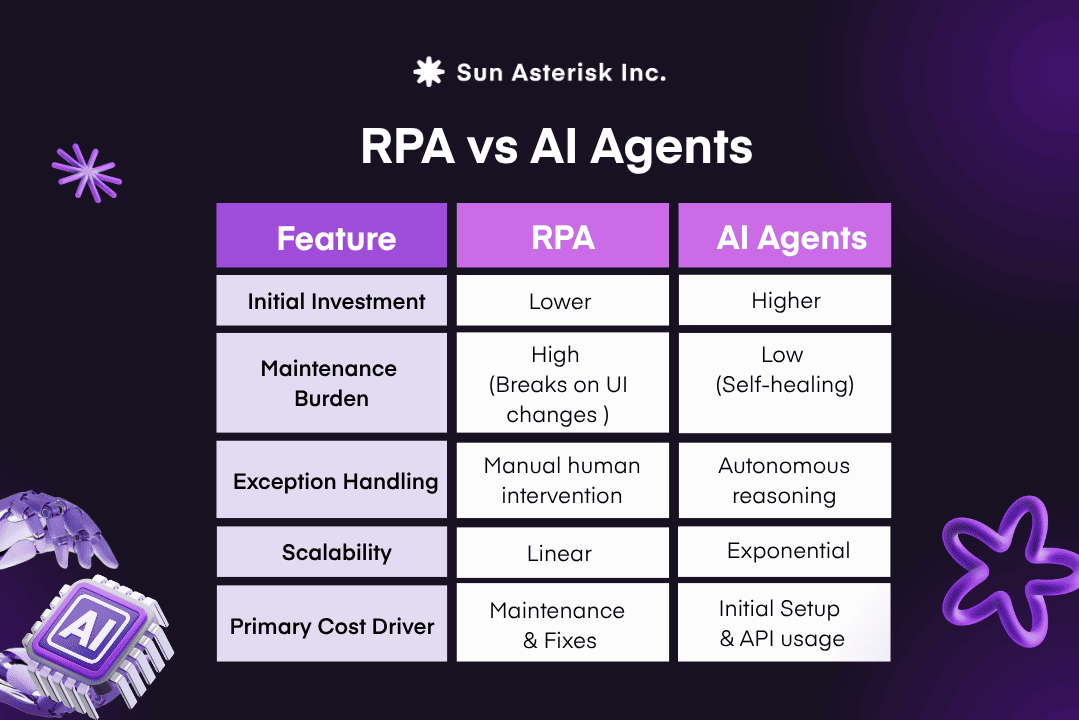
In practice, the RPA vs. AI agents debate is where most mid-sized clinics get stuck. RPA has a longer track record. AI-powered automation is newer, more capable, and often more expensive upfront. Choosing the wrong approach doesn’t just waste budget-it can quietly increase the healthcare workflow automation cost by adding maintenance overhead and operational friction.
Our advice: stop focusing on setup cost alone and start looking at the Maintenance Tax. That’s where the real healthcare workflow automation cost reveals itself. In this article, we’ll break down how to evaluate each option properly and what the right decision looks like for a clinic your size.
Read more: Build vs Buy: How to Calculate the True Cost of Healthcare IT Outsourcing
Key Summary
- RPA is cheaper to start, but AI is cheaper to run: While RPA is cheaper to start, AI agents cut more costs over time by autonomously handling the 20% of clinical “exceptions” (like portal updates or messy data) that typically break rigid scripts.
- Focus on Outcome-Driven Automation: AI agents reduce human administrative work by up to 60% because they can “read” unstructured documents and manage complex tasks like Prior Authorization, whereas RPA requires constant manual fixing.
- Adopt a Hybrid Model: For 2026, the most cost-effective clinics use RPA for simple data syncing while letting AI act as the “brain” to orchestrate workflows and manage decision-heavy tasks.
How AI Agents differ from RPA in a practical clinical context?
The most direct way to evaluate these tools is to look at how they actually perform on the clinical front lines—because that’s where the true healthcare workflow automation cost becomes visible.
RPA functions by mimicking discrete human actions like clicking buttons, filling forms, and syncing data across interfaces. It is a disciplined, literal digital worker that excels at following a rigid script.
However, the moment a payer portal updates or a new field appears in your EHR, that script fails. RPA stops and waits for human intervention.
Goal-driven AI systems offer a significant advancement. Unlike systems requiring a predefined map for every scenario, an AI-powered system can autonomously manage complex, unstructured tasks. For instance, it can process an unstructured referral, identify missing clinical data, and initiate necessary follow-ups without manual workflow redesign.
This ability allows it to reason through ambiguity, adapt to changes and maintain workflow continuity without needing human intervention every time a situation deviates from the expected script.
Over the past 18 months, the practical gap between these two approaches has widened into a chasm, and in the high-stakes environment of healthcare, this gap is the difference between true scalability and growing technical debt.
Why healthtech leaders underestimate the true cost of running clinics with RPA?
RPA had its moment. For stable, high-volume, rule-based processes, think billing code entry for a single payer, or nightly appointment reminders via a fixed template, it delivered strong early ROI. Implementations moved fast, licensing was affordable, and the demos were impressive. On paper, RPA gets you to your first automation in 3-6 months and looks like the sensible, low-risk choice.
RPA’s ROI is real but only early. Most clinics see returns plateau or decline after the first 6 -12 months as maintenance demands compound and workflow complexity grows.
AI-powered automation, by contrast, reduces human escalations because it handles exceptions on its own rather than stopping and waiting. It takes longer to reach breakeven, roughly 6 to 12 months versus RPA’s 3 to 6 but it doesn’t plateau. The savings compound as your clinic scales.
How AI agents reduce healthcare workflow automation cost by handling what RPA can’t
RPA’s core limitation isn’t cost or speed, it’s that it can only follow scripts. Clinical workflows don’t follow scripts.
In prior authorization, an RPA bot only works when every field matches perfectly. The moment something changes, such as missing clinical notes, a portal outage, or a requirement to switch to fax, it fails. It cannot assess the situation or adapt, it simply stops.
An AI agent approaches the same scenario differently. It can read denial letters, understand the reason for rejection, gather the necessary supporting documents from patient records, draft a resubmission, and route it for a physician’s signature as one coherent process. It also applies in a clinical context, recognizing when a patient may qualify for a policy exception based on newly documented conditions.
This capability extends beyond prior authorization. In most mid-sized clinics, critical clinical data is fragmented across EHR notes, scanned PDFs, lab results, and referral letters. While RPA depends on clean and structured inputs, AI agents can synthesize this fragmented information into a complete and usable view of a case without manual consolidation.
When unexpected changes occur, such as policy updates, interface changes, or unanticipated edge cases, AI agents can adapt or escalate intelligently instead of failing silently. As a result, they can reduce human escalations by up to 60% compared to RPA systems handling similar workloads.
This is the fundamental shift from automating individual steps to automating outcomes.
Which Automation makes sense for Mid-sized Clinics in 2026?
Most clinics think they need automation, but the real challenge is choosing the right type for how their operations actually work. For mid-sized clinics in 2026, the answer is less about picking a single tool and more about understanding which approach delivers the most value across different parts of the workflow. Most cost comparisons stop at the license fee. The ones that actually inform a good decision go further, across 04 dimensions that don’t appear on any vendor proposal.
| Cost Dimension | RPA | AI-Powered Automation |
|---|---|---|
| Implementation Cost |
Lower
Faster setup, minimal integration. Advantage is real for stable, simple workflows. |
Higher
More scoping and multi-source integration are needed. Cost justified by long-term returns. |
| Maintenance Cost |
High
Every UI change breaks the bot. Typically, 15–25% of implementation cost annually. |
Low
Adapts to variation without a rewrite. Understands intent, not just screen layout. |
| Staff Time Saved |
Partial
Automates predictable steps, but a human still handles every exception. |
Higher
Reduces exception volume by up to 60%, freeing staff from bot babysitting. |
| Error Cost |
Elevated
Stale data causes silent failures (billing rejections, compliance flags). |
Lower
Reasons from context, catches inconsistencies before submission. |
Once you understand the full cost picture, the decision becomes less about budget and more about fit—specifically, which technology aligns with the actual nature of your workflows. That’s the only way to accurately assess your long-term healthcare workflow automation cost.
The clearest signal is your exception rate. If more than 10-15% of your automated cases require a human to step in and fix something, it’s a technology mismatch.
RPA was not designed for clinical environments where payer rules change quarterly, patient data arrives incomplete, and no two prior auth cases look exactly alike. Forcing it to handle that complexity doesn’t make your clinic more efficient, it just moves the manual work from one place to another.
On the other hand, if your target workflow is genuinely simple: nightly appointment reminders, a single-payer eligibility check, or a fixed data sync between two stable systems, RPA will get the job done faster and at lower upfront cost than any AI-powered alternative.
The mistake most clinics make is applying a $100K solution to a $20K problem, or worse, applying a $20K solution to a $100K problem. Know which one you have before you buy anything.

Hybrid RPA and AI architecture to reduce healthcare workflow automation cost
The most practical path for most mid-sized clinics in 2026 is not a full rip-and-replace of existing automation.
It is a two-layer architecture. RPA handles the stable, rule-based execution tasks it was built for, such as form pulls, API calls and data syncs while AI-powered automation sits above it as the orchestration layer.
This orchestration layer decides when to trigger those bots, handles exceptions, and manages every step that requires judgment or contextual reasoning.
Think of it as the brain directing the hands.
The right place to start is one high-friction workflow, not your entire operation. Prior authorization is the most proven entry point. It consumes up to 13 hours of physician time per week, causes 3 to 7 day care delays, and involves exactly the unstructured payer logic that breaks RPA.
An AI-powered system handles the full cycle autonomously and reduces decision timelines from days to minutes. Revenue cycle management is the next highest-impact target, with real-world deployments demonstrating up to a 292% ROI and a 40% reduction in FTE administrative requirements.
The design principle that separates successful deployments from expensive ones is knowing where to keep humans in the loop. Auto-approve high-confidence routine cases. Flag complex edge cases below 70% confidence for physician review.
This is not a workaround for limitations in the technology. It is the architecture of a compliant, trustworthy system that your clinical team will actually adopt.
3 key questions to evaluate RPA vs AI agents and optimize healthcare workflow automation cost
If you’re evaluating automation for your clinic right now, here are the 03 questions worth answering before you decide anything:
1. What percentage of your target workflows involve exceptions, ambiguity, or unstructured inputs?
If it’s over 20%, RPA will disappoint you. Start with AI-powered automation for those workflows.
2. What’s your actual 3-year budget, not just the initial implementation?
Get a maintenance cost estimate in writing from your RPA vendor. Compare that to the agent platform’s total cost projection. The gap is usually more than you expect.
3. Do you have the internal capacity to manage Bot failures?
RPA requires ongoing human oversight. If your IT team is already stretched, every bot failure becomes a staffing problem. AI-powered automation reduces that dependency substantially.
Find the right Automation approach for your clinic
If you want to run the numbers on your specific workflows where RPA starts to break and where AI-powered automation begins to reduce cost, our AI experts at Sun* can walk you through it, based on your current admin stack and real operational data.
Need help assessing workflow automation cost? 👉 Book a free consultation