As of 2026, Agentic AI is the new cool guy in healthcare. By now, we’re all talking about agentic AI in healthcare, but here is the reality check: AI agent interoperability is currently slamming into a brick wall built in the early 2000s.
For most health systems we’ve worked with, the greatest barrier to this future isn’t the AI itself; it’s the Electronic Health Record (EHR).
While modern agentic logic is built for the cloud, real-time APIs, and fluid data, our legacy EHRs were built as static digital filing cabinets. They are robust for billing and record-keeping, but they were never designed to host an autonomous “digital team member.”
Working with our clients, we’ve seen that the “Agentic leap” often lands on the jagged rocks of legacy infrastructure.
Here are the 5 critical challenges healthcare leaders must navigate to integrate agentic logic without destabilizing their core operations.
The principal-agent paradox of 2026
The clinicians (the principals) are desperate for their “software destiny”—the right to use autonomous tools that actually solve burnout. Yet, the IT decision-makers (the agents) are protecting a legacy system of record that has become a system of control.
1. The AI agent interoperability mountain to climb: capability vs. access
In the current landscape of AI agent interoperability, we are seeing a fundamental clash between two different eras of computing.
Nowadays, HL7 FHIR (Fast Healthcare Interoperability Resources) has become the global standard.
Yet, even with widespread adoption, legacy EHRs often implement FHIR as a “read-only” or “batch-driven” layer rather than a truly bidirectional interface.
It’s the main challenge here: Agentic AI requires more than just access to data; it requires the ability to write back to the EHR and trigger subsequent clinical actions (like ordering a lab or updating a care plan).
Many legacy systems still rely on proprietary, non-standardized data schemas beneath their FHIR wrappers. When an AI agent attempts to execute a multi-step workflow such as coordinating a referral, it often hits a wall where the legacy API cannot support the specific “write” operation required.
What should you do? Leaders must move toward modular integration layers.
Instead of trying to force the agent to speak directly to the legacy EHR, we build “wrapper” services that normalize proprietary data into actionable agentic prompts.
Don’t wait for your EHR vendor to catch up; build the abstraction layer your agents need to thrive.
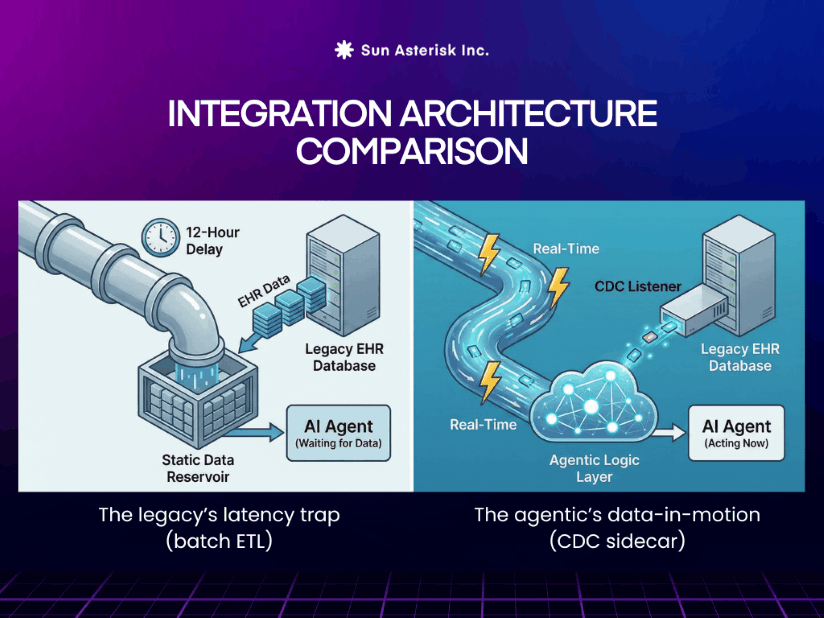
2. The latency gap: real-time logic vs. batch processing
The core challenge here is a synchronization problem.
Most legacy systems rely on nightly ETL (Extract, Transform, Load) cycles or high-latency batch processing that refreshes data in intervals of minutes or even hours.
Agentic AI operates on an Event-Driven Architecture (EDA). It needs to “hear” a patient’s request, “sense” a drop in vitals, and “act” immediately.
Legacy EHRs, however, often rely on batch processing refreshing data in intervals of minutes or even hours.
If your AI agent is managing a post-discharge patient and needs to intervene when a biometric alert is triggered, a 15-minute sync delay from the legacy system is an eternity. This “latency gap” means the agent is making decisions based on “stale” data and it creates a significant clinical and legal liability.
In a live medical environment, a “near real-time” agent is often just an agent waiting to make a mistake.
📍Did you know? Recent industry research indicates that nearly 40% of agentic AI projects are projected to fail by 2027, primarily because teams underestimate the infrastructure upgrades needed to support autonomous workflows.
Our proposed solution to the AI agent integration latency gap
To achieve a true return on investment, leaders must move their infrastructure from “Data-at-Rest” to Data-in-Motion.
By implementing Change Data Capture (CDC) on legacy databases or leveraging event-mesh technology, you can “push” updates to the agentic layer the microsecond they occur.
This allows the AI to function as a truly autonomous partner, reacting to business and clinical events as they happen rather than waiting for the next batch job to run.
True AI agent interoperability requires a “live heartbeat”. If your agentic logic is sprinting while your legacy EHR is walking, the resulting data lag will eventually submarine your most ambitious AI initiatives.
3. The “chained vulnerability” risk in legacy security
Legacy EHRs were built with a “Perimeter Security” mindset. It keeps everyone out who doesn’t have a login.
Agentic AI, however, requires system-to-system autonomy, where agents talk to other agents, insurance portals, and pharmacy systems.
The challenge: Integrating an autonomous agent into a legacy system creates a “Chained Vulnerability.”
If an agent is compromised, it has the potential to move laterally through the legacy pipes that were never designed for internal segmentation.
Furthermore, legacy systems often lack the granular Identity and Access Management (IAM) needed for agents.
Does the agent have “physician-level” permissions? If so, how do you audit a machine that executes 1,000 tasks per second?
What’s the solution to healthcare legacy security? Implementation of Agentic Zero Trust.
Treat every AI agent as a unique identity with its own ephemeral credentials and strictly limited “Least Privilege” access.
You must implement robust audit logging that captures not just the result of the agent’s action, but the reasoning (chain of thought) behind it.
4. Governance and Human-in-the-Loop friction
Moving from “Assisted AI” (which suggests) to “Agentic AI” (which acts) requires a massive leap in clinical governance. Legacy EHRs offer almost no native support for managing autonomous decision-making.
In large healthcare enterprises, clinicians often feel they have lost their “software destiny.” While an individual doctor might see an agentic scribe or a coding copilot as a lifeline, the enterprise hierarchy frequently views any non-certified, autonomous interaction with the EHR as a high-stakes security threat.
This friction is compounded by a lack of native support in legacy EHRs for managing agentic AI (which acts) versus assisted AI (which merely suggests).
When an agent autonomously schedules a follow-up or pulls context from a “free-text” note, the question of liability looms large: Who is responsible if the agent misses a critical nuance buried in unstructured legacy data?
Without deterministic guardrails, a “black box” agent operating within a legacy environment is viewed as an unacceptable risk by the gatekeepers of the enterprise.
Note for leaders: turn shadow AI to formal governance

If this divide is not bridged, organizations face the rise of what we’ve called “shadow AI,” where frustrated clinicians bypass official channels to use unauthorized tools, creating massive data leakage and compliance risks.
Recent data suggests that while over 88% of health systems use AI internally, only 18% have a fully formed governance strategy.
Leaders must pay attention because the “No” culture of the past is no longer a viable risk-management strategy; it is a recipe for operational fragmentation and clinician burnout.
Our AI agent interoperability fix is to build governance as a feature
From our experience in healthcare project as a healthcare IT outsourcing partner, leaders must move toward a tiered autonomy model powered by a Human-in-the-Loop (HITL) framework.
Instead of treating the agent as a hidden back-office script, we advise deploying orchestration dashboards that sit above the legacy EHR.
These dashboards act as a “governance tier,” where the agent proposes an action—complete with its reasoning and data sources—and waits for a clinician’s “one-click approval” before committing the data back to the EHR record.
This approach satisfies the CSO’s need for oversight while giving the clinician the speed and support they require. Start by granting full autonomy only in low-stakes administrative areas (like prior-auth prep or basic scheduling) while keeping clinical logic in the shadow mode until confidence thresholds are consistently met.
5. Final challenge: the shadow integration trap of velocity and vitality
Startups and SMBs practices are increasingly sidestepping cumbersome EHR developer programs and brittle, “read-only” APIs by deploying Agentic RPA.
By utilizing advanced computer vision, these agents “see” and “click” through the legacy interface exactly like a human would. This allows for massive velocity, enabling organizations to deploy sophisticated automation in weeks rather than the months required for traditional AI agent interoperability through certified pathways.
However, this high-velocity bypass comes with a significant technical and cultural debt.
On the technical side, it creates a maintenance trap where a single UI update from an EHR vendor can break an agent’s logic overnight, turning a productivity tool into a system-wide failure.
On the cultural side, we are seeing a profound trust deficit (skepticism) fueled by implementation trauma.
What is it about?
Healthcare staff have spent a decade fighting with their EHRs; the idea of an autonomous agent “doing work for them” is often met with deep skepticism.
Clinicians don’t want a “new tool”; they want their existing EHR to work better.
When agentic logic “hallucinates” or makes a mistake in a legacy field, it reinforces the trust deficit, leading to abandonment of the technology.
Our suggestion for AI integration in your legacy
Leaders, focus on Workflow-Native UI. The agent’s actions must be visible within the EHR’s native view.
For leadership, the risk of a shadow integration is that it often solves for speed at the expense of long-term vitality.
If an agent is poorly integrated, requiring clinicians to verify actions in a separate window, it will eventually be abandoned as “too much work.”
If the agent drafts a note, it should appear in the “Drafts” section of the legacy EHR, not in a separate window. Success in 2026 is measured by how “invisible” the agent feels to the end-user.
Your path to an agentic future
The transition from the “Static EHR” to the “Agentic Care Ecosystem” is the defining challenge for healthcare leadership in 2026. You cannot wait for legacy vendors to modernize their core at the speed of AI.
You must build the integration, security, and governance layers today that will allow agents to navigate your legacy environment safely and effectively.
At Sun*, we help organizations build FHIR-native, agent-ready architectures that “unlock” legacy EHRs without requiring a total system replacement. From real-time data streaming to secure multi-agent orchestration, we provide the technical expertise to turn your legacy debt into a competitive engine.
🔋 Book an Architecture Readiness Audit with our team today, and let us help you map the real-time pipelines and governance guardrails your agents need to thrive.