Automating workflows in EHR systems is no longer optional. Learn how agentic AI helps healthcare leaders eliminate admin burden, not just reduce it.
EHR workflow automation isn’t a theoretical problem. It’s a response to physician burnout, rising administrative cost, and systems that added documentation work instead of removing it.
We focus on the next inflection point: moving beyond pilots and point AI tools toward rebuilding the EHR’s administrative layer with autonomous agents.
In this article, we’re going to explain the real difference between ambient AI and agentic AI, highlight 05 clinical workflows with the strongest automation ROI, and provide a practical framework for turning the EHR from a documentation burden into a self-managing clinical operating system.
Ambient AI reduced documentation time, but someone still has to proofread, approve, and file every output. Agentic AI goes further: autonomous agents that execute scheduling, coding, prior authorization, and referrals end-to-end, without clinician intervention at every step. That is the difference between shifting the administrative burden and actually eliminating it.
The “Invisible AI” Imperative – What Healthcare Leaders Actually Want
Defining “Invisible AI” in clinical workflow
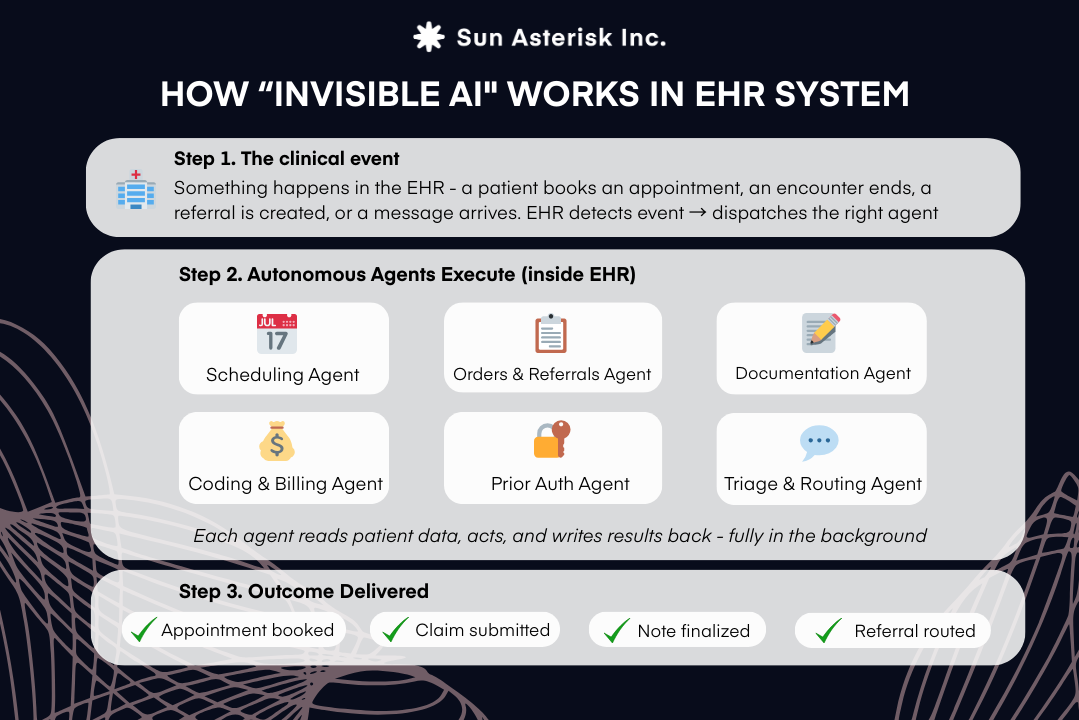
In clinical settings, “invisible AI” refers to artificial intelligence that operates entirely in the background of the EHR: triaging patient messages, scheduling appointments, coding encounters, routing orders without requiring the clinician to interact with a menu, open a module, or review an output before it is filed.
The clinician neither sees the AI working nor is asked to intervene. It simply happens.
A real-world example illustrates this well: Epic’s ambient documentation integration with DAX Copilot (Microsoft Nuance).
When a physician walks into an exam room, the system automatically begins listening. By the time the encounter ends, a structured SOAP note complete with ICD-10 code suggestions and relevant HCC capture flags, is already populated inside the physician’s Epic chart, ready for a single-click attestation.
The doctor never opened a documentation app, never typed, never dictated. The EHR simply did it.
Why is “invisible” the goal?
Healthcare leaders are not asking for smarter tools. They are asking to stop thinking about tools at all.
Every click, every review prompt, every approval modal is a cognitive interruption that pulls a physician’s attention away from the patient in front of them. The ideal AI doesn’t augment the physician’s administrative life; it removes it.
A 2025 survey by SS&C Blue Prism found that 94% of healthcare organizations now view AI as core to their operations, and 86% are using AI extensively. A signal that the question is no longer whether to automate but how deeply to automate.
Why “Listening-Only” AI is Not Enough
Ambient AI documentation tools, sometimes called AI voice agents in clinics or ambient scribes, have been the dominant AI story in healthcare for the past two years.
The adoption numbers are striking: a 2025 study found that nearly two-thirds of U.S. hospitals on Epic EHR systems have deployed ambient AI tools. And the clinical satisfaction data is genuinely positive.
These are meaningful, defensible results. So what is the problem?
The problem is what ambient AI leaves behind.
Ambient scribes generate draft notes, but someone must still review them. That task, invisible in the ROI calculations, creates a new category of work researchers call “unnamed tasks”: proofreading AI-generated text, correcting specialty-specific terminology, editing for medicolegal accuracy, and attesting in the chart.
A rapid review published in JMIR AI found that while ambient tools produced “consistent reductions in documentation time,” they did not significantly change burnout levels, and key areas, including “cost-effectiveness, care quality, and safety concerns such as transcription errors and fabricated content were infrequently addressed.”
Ambient scribes reduce typing but not workload by shifting documentation into “unnamed tasks” like proofreading and attestation. They deliver time savings without meaningfully improving burnout or addressing cost, quality, and safety risks.
Why Automating Workflows in the EHR Is the Only True Solution
The fundamental problem is that ambient scribes treat documentation as an output – a note to be generated. But clinical documentation is actually an input to a much larger workflow: scheduling, coding, referrals, authorizations, and billing. When AI only optimizes the note-writing step, it leaves every downstream step untouched.
True relief requires automating workflows in EHR systems end-to-end: not just drafting the note, but using the contents of that note to automatically trigger the next five steps in the care pathway, before the clinician ever thinks to initiate them.
The Shift From Ambient to Agentic AI in Healthcare
The industry is now undergoing a generational transition in how AI is applied to clinical operations, moving from tools that listen and suggest to agents that reason and act.
Ambient AI captures conversational data and converts it to structured text. It is a listening and transcription layer. The clinician still reviews, edits, and signs. The AI is essentially a very good scribe.
Agentic AI is fundamentally different in architecture and ambition. An AI agent maintains a goal, breaks that goal into a sequence of steps, calls external tools and APIs, verifies its own outputs, and adapts when conditions change, all without a human initiating each step.
In healthcare, this means an agent can receive a patient referral, check insurance eligibility, determine whether prior authorization is required, pull relevant clinical history from the EHR, draft and submit the authorization request, monitor payer response, and update the care team, without a single staff member touching the file.
The market is reflecting this shift with remarkable speed. The global agentic AI in healthcare market was valued at $538.51 million in 2024 and is projected to reach $4.96 billion by 2030, growing at a CAGR of 45.56%.
Healthcare executives are paying attention.
A September 2025 Deloitte survey of 100 U.S. healthcare technology leaders found that 40% said technical talent limitations are no longer a major adoption barrier, and 38% reported reduced friction from change resistance, signals that agentic AI is moving from experimentation into operational scale.
For healthcare leaders, the strategic question is no longer whether to invest in AI automation, but where to deploy agentic capability first and how to sequence the rollout for maximum ROI.
What Workflows Can Actually Be Automated in EHR Systems
Defining Automation in Clinical Workflows
Clinical workflow automation is the use of software, increasingly AI-driven, to execute defined sequences of tasks within or across health IT systems without requiring manual input at each step.
In the EHR context, automating workflows in EHR systems ranges from simple rule-based triggers (e.g., “when a patient checks in, update the intake status”) to sophisticated agentic processes that span multiple systems, interpret unstructured clinical text, and make real-time decisions based on payer rules, patient history, and clinical protocols.
True automation is end-to-end: it begins with a clinical event, completes the associated administrative and clinical follow-up tasks, and writes the outcomes back to the system of record with appropriate human checkpoints for high-stakes decisions.
Key Use Cases for Automating Workflows in EHR Systems
1. Automated Clinical Scheduling
Manual scheduling is one of healthcare’s most persistent inefficiencies. Phone-tag with patients, double-booking, no-show management, and complex multi-specialty coordination consume enormous staff time.
AI voice agents in clinics can conduct outbound and inbound scheduling calls autonomously: confirming appointments, handling rescheduling requests, managing cancellation waitlists, and sending reminders via SMS or email. All integrated directly with the EHR’s scheduling module.
Agentic systems can also auto-prioritize appointment slots based on clinical urgency flags in the patient record.
2. Orders & Referrals
Referral management is a notorious gap in care continuity. Patients fall through the cracks between the moment a referral is placed and when the specialist receives complete clinical context.
Agentic AI monitors order queues in the EHR, identifies referral orders, automatically assembles the relevant clinical documentation (notes, lab results, imaging reports), matches the patient to the appropriate specialist based on payer network, geography, and availability, and routes the referral electronically. The referring provider is notified only when specialist confirmation is received or if an exception requires escalation.
3. Clinical Documentation & Note Finalization
Agentic documentation goes further by not merely drafting notes but finalizing structured data fields based on note content.
An agentic documentation system listens to the encounter, drafts the narrative note, populates structured EHR fields, suggests and pre-populates orders aligned with the clinical narrative, and flags any quality measures due for the patient. All before the clinician opens the chart post-visit.
Ambient AI with deep EHR integration reduced documentation time by 30 minutes per day per provider and improved note accuracy for diagnosis billing, a combination that generates both time savings and revenue recovery.
4. Medical Coding & Revenue Cycle
Medical coding is one of the most labor-intensive and error-prone steps in the revenue cycle. Incorrect or incomplete coding results in claim denials, revenue leakage, and compliance risk.
AI coding engines analyze clinical documentation in real time, suggest appropriate ICD-10, CPT, and HCC codes, identify documentation gaps that would support higher-acuity codes, and pre-populate the billing interface before the coder reviews the chart.
Autonomous Admin Agents can take this further by submitting clean claims directly to the clearinghouse, monitoring for rejections, and automatically correcting and resubmitting based on payer-specific rules.
5. Prior Authorization & Insurance Workflows
Prior authorization (PA) is widely regarded as the single most disruptive administrative burden in clinical medicine.
When an order that requires prior authorization is placed in the EHR, an agentic AI system immediately detects the PA requirement.
It retrieves the patient’s insurance eligibility and benefit details directly from the payer record.
The agent then assembles the necessary clinical documentation from the encounter, orders, and history.
The economics of automation here are striking.
According to Intersystems, manual prior authorization costs an average of $3.68 per request when accounting for staff time, portal access, and follow-up calls. Automated prior authorization costs approximately $0.04 per request.
Industry analysis indicates that 80% of prior authorizations requiring clinical and administrative review can be fully automated using current AI and FHIR-based API infrastructure.
Our vision: “The EHR is the OS, AI is the App”
At Sun*, we believe the future of healthcare technology follows a specific architecture: The EHR should serve as the Operating System (OS), while AI serves as the “App” or “Agent” that runs on top of it.
AI’s role is to extend that foundation. Like apps on a smartphone, agentic AI systems don’t rebuild the OS; they unlock new capabilities on top of it.
Operating at machine speed, coordinating across departments, and acting continuously after each encounter, AI can execute work no human-staffed workflow can sustain.
This belief drives how we build. By automating workflows in EHR systems, we embed AI inside the EHR’s security, data, and audit model, not beside it. We design agents as modular, swappable capabilities, not a monolithic platform.
And we make humans governors, not gatekeepers, providing oversight through audits and exceptions, while AI handles routine execution autonomously.
When done right, the result is simple: clinicians practice medicine and go home. Scheduling, documentation, coding, authorizations, and referrals happen automatically, inside the EHR, triggered by care itself.
Ready to Take the Next Step?
Whether you are evaluating your first AI workflow automation pilot or scaling from proof-of-concept to enterprise deployment, the strategic principles are the same: start with the highest-friction workflows, build natively inside the EHR, and measure ROI on clinician time, denial rates, and authorization turnaround, not just user satisfaction scores.